
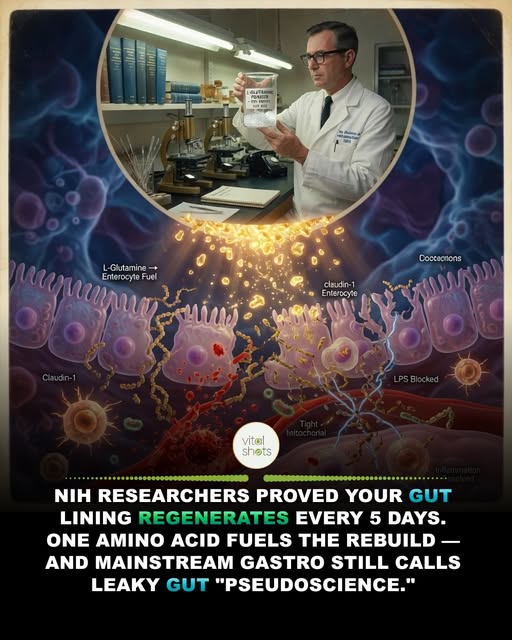
In 1974, a research team at the National Institutes of Health published a quiet observation that should have rewritten clinical gastroenterology. The cells lining the human small intestine — called enterocytes — are among the most metabolically active cells in the entire body. They turn over completely every three to five days. They regenerate constantly, faster than any other tissue except bone marrow. And they have one unusual property no other cell type shares: their primary metabolic fuel is not glucose. It is the amino acid L-glutamine.
This was confirmed in animal studies, then human surgical patients, then bone marrow transplant recipients whose gut barriers had been destroyed by chemotherapy. Every time, the same finding: when L-glutamine was supplemented, gut barrier integrity restored measurably. When it was withheld, the gut lining thinned and leaked.
For five decades, this research has remained quietly accumulating in surgical, oncological, and critical care literature. Yet mainstream gastroenterology continued to dismiss “leaky gut” — the popular term for intestinal hyperpermeability — as a pseudoscience marketing concept. Functional medicine practitioners who acknowledged the science were dismissed as unscientific. The pharmaceutical industry built no drugs around the L-glutamine pathway because the molecule is endogenous and unpatentable.
Meanwhile, the same intestinal permeability that mainstream medicine refused to name began to be reluctantly acknowledged under the more clinical label “increased intestinal permeability” and its connection documented to autoimmune disease, food sensitivity, chronic inflammation, brain fog, joint pain, skin disorders, and even depression through the gut-brain axis.
L-glutamine acts on three independent pathways simultaneously. It is the direct fuel source for enterocyte ATP production — the cellular energy required for active tight junction protein synthesis. It is a substrate for glutathione production — the body’s primary antioxidant defense that protects intestinal cells from oxidative damage. And it directly upregulates the expression of claudin and occludin proteins — the structural proteins that physically clamp adjacent enterocytes together to form the tight junction barrier.
Without sufficient L-glutamine, all three pathways collapse together. The intestinal lining cannot generate the energy to maintain itself, cannot defend against oxidative damage, and cannot synthesize the structural proteins of the barrier. The gut leaks. Endotoxins enter the bloodstream. Systemic inflammation rises.
Hospital pharmacies stock IV L-glutamine for burn patients, surgical recovery patients, and chemotherapy-induced gut damage. Functional medicine clinics use oral L-glutamine for autoimmune protocols, food sensitivity reversal, and post-antibiotic recovery. The data is identical. The institutional acceptance is not.
Rebuild the gut wall:
– The 5g / Twice Daily Floor: Therapeutic oral L-glutamine starts at 5 grams twice daily — taken on an empty stomach in 8 oz of water. Lower doses produce maintenance effect; serious gut barrier repair requires the higher window. Some clinical protocols extend to 10 g twice daily for acute autoimmune flare-ups.
– The Empty Stomach Rule: L-glutamine competes with other amino acids for intestinal absorption. Take it 30 minutes before meals or 2 hours after, with nothing but water. Mixing with protein meals dilutes the targeted delivery to enterocytes.
– The Zinc Carnosine + Slippery Elm Stack: The fastest gut barrier repair protocol combines 5 g L-glutamine + 75 mg zinc carnosine + 1 teaspoon slippery elm bark powder, taken twice daily for 8-12 weeks. This is the protocol used in integrative gastroenterology clinics in Sydney and Vienna. It outperforms PPI medications for symptom relief and addresses the underlying barrier defect rather than suppressing acid.
Journal of Parenteral and Enteral Nutrition. “Glutamine metabolism and the gastrointestinal tract”.
Annals of Surgery. “Glutamine supplementation in critically ill patients: clinical trials and outcomes”.