
“Definiteness of purpose is the starting point of all achievement.”
W. Clement Stone – Author (1902 – 2002)
Here’s Why He Paid $25,000 For This Advice
Watch video: https://www.youtube.com/shorts/83v2nd99BWU
Here Is What I Do
What Happens When You Reintroduce An Apex Level Predator?

In June 1999, the Smithsonian Institution initiated a controversial predator reintroduction project that would fundamentally change the field of island biogeography. By releasing two captive-bred harpy eagles onto Barro Colorado Island—a tropical forest isolated by the creation of the Panama Canal—scientists sought to restore an ecosystem that had been aging in silence without an apex predator for eighty-five years. What followed was not a predictable ecological study, but a brutal demonstration of evolutionary adaptation that shattered every mathematical model.
This nature documentary uncovers the phenomenon known as the landscape of fear, revealing how target prey populations rapidly altered their genetics, vocalizations, and behavior to survive an aerial ambush. From the specialized hunting mechanics of the harpy eagle to the bizarre defense strategies of native monkey troops using humans as shields, discover why this top-down conservation experiment became too intense to allow to continue.
Click to view the video: https://www.youtube.com/watch?v=ga0x8Uuum4g
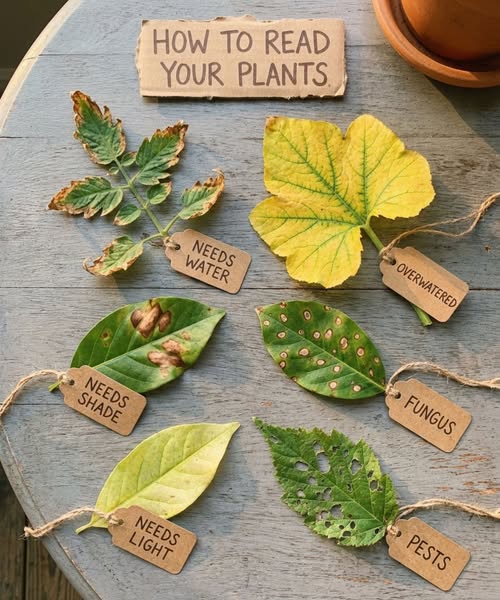
Leaf Diagnosis
The Dark Story of the Comeng Train Factory

How to destroy a country’s manufacturing ability. A Case History.
The major point this video fails to make is that all Australia’s political leaders since the 1972 Lima Agreement have been complicit in the destruction of industry. I read that the reasoning behind the Lima Agreement was that no country should be able to stand alone against global coercion and that if a single country had mineral wealth, mining capacity, manufacturing capability and food self-sufficiency they were harder to push around.
Our ‘leaders’ (read ‘traitors’) blew it big time!
Click to view the video: https://www.facebook.com/reel/1042529858532510
Elif Shafak
She gave birth to her first child and five days later a courtroom decided whether her words would cost her three years of freedom.
Her name was Elif Shafak. The year was 2006. Shafak was lying in an Istanbul hospital bed, unable to attend her own trial, when the verdict arrived.
The charge was insulting Turkishness. The evidence was dialogue spoken by fictional characters in her novel.
Remember that. The characters were not real. The prosecution was.
Shafak was born in 1971 in Strasbourg, France, to Turkish parents who separated when she was still an infant. Her mother brought baby Shafak back to Ankara and did something unusual for a woman of her generation — she returned to university, finished her degree, then joined the Turkish foreign ministry.
Shafak grew up in a household without a patriarch. Her grandmother filled the space with stories instead — reading coffee cups, burning lead to ward off the evil eye, passing down oral traditions that official Turkey preferred to forget. Young Shafak started keeping a diary at eight years old. Her own life felt too ordinary to write about, so she started inventing people who didn’t exist.
At 10, her mother’s diplomatic posting carried them to Madrid. Shafak was the only Turkish student at her new school, scrambling to learn Spanish fast enough to survive. She was bullied. She was lonely. Then, as a teenager, she discovered Don Quixote in its original Spanish — a book, she later said, that shook and completely changed her.
Books became her passport out of isolation.
After earning degrees in international relations and gender studies, then a doctorate in political science, Shafak became a novelist, writing about the hidden histories Turkey’s official narratives preferred to bury.
Her 2006 novel, “The Bastard of Istanbul,” went furthest. It followed two families — one Turkish, one Armenian-American — connected by secrets buried across generations. In it, fictional Armenian characters discussed the mass killings of Armenians during World War I using a word the Turkish government had long forbidden: genocide.
For that, Shafak became the first author ever charged under Article 301 of Turkey’s penal code specifically over the words of fictional characters rather than her own personal statements. She faced up to three years in prison.
Outside the courthouse on the day of her trial, ultranationalists burned European Union flags and spat on photographs of her face. Inside, her lawyer defended her fictional Armenian characters as though their perspectives mattered — as though fiction itself were on trial.
It was.
The case dragged on for months. Shafak waited, pregnant, not knowing whether she would give birth in freedom.
She did. And five days after delivering her daughter, the verdict arrived at her hospital bedside.
The prosecutor asked for the charges to be dropped. Shafak was acquitted.
Here is what most people miss: acquittal doesn’t undo the fear. The crowds who spat on her photographs didn’t disappear. The chill that falls over a writer who has watched a courtroom debate the words of her invented characters doesn’t simply lift because a judge says not guilty.
Thirteen years later, it happened again.
In 2019, Turkish prosecutors investigated Shafak for obscenity — this time over depictions of sexual violence in her novel “10 Minutes 38 Seconds in This Strange World,” a book that had just been shortlisted for the Booker Prize, telling the story of a murdered sex worker in Istanbul.
Shafak pointed out the bitter irony herself. The courts were not acting to prevent actual violence against women and children. They were prosecuting the writer who depicted it.
“It has become like a witch-hunt,” she said.
The personal cost across two decades was real. Legal proceedings. Public harassment. Exile from the country whose stories she had devoted her life to telling.
Shafak kept writing anyway.
Elif Shafak now lives in London, writing in both Turkish and English, her novels translated into nearly 60 languages and read by millions who will never see a courtroom over her words.
“To be a novelist in Turkey,” she has said, “is a heavy experience. Overnight, you can find yourself almost digitally lynched.” And yet, she adds, stories matter most precisely in places where democracy is fading.
Fiction doesn’t escape reality. It confronts it. That is exactly why it frightens the people determined to control the story.
One hospital bed. One newborn daughter. One acquittal that came too late to undo the fear. One second prosecution thirteen years later. Nearly 60 languages carrying her words past every border built to stop them.
They called Elif Shafak dangerous.
She has spent every year since proving them right — in exactly the way that matters.
Tag someone who believes the most important stories are the ones they try hardest to silence. Like and share for Elif Shafak — because words that frighten power are exactly the words worth keeping.
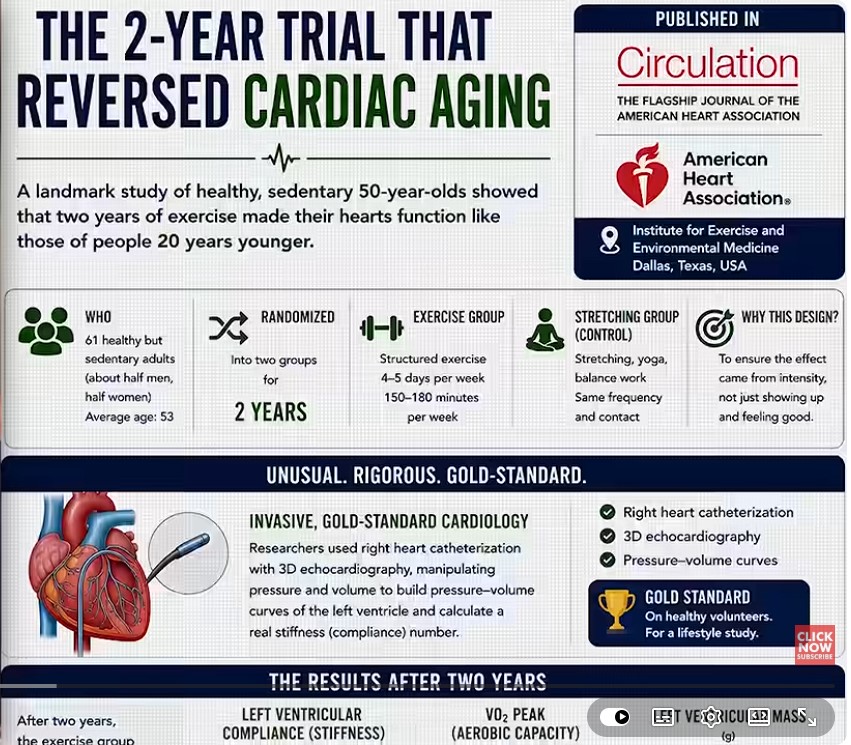
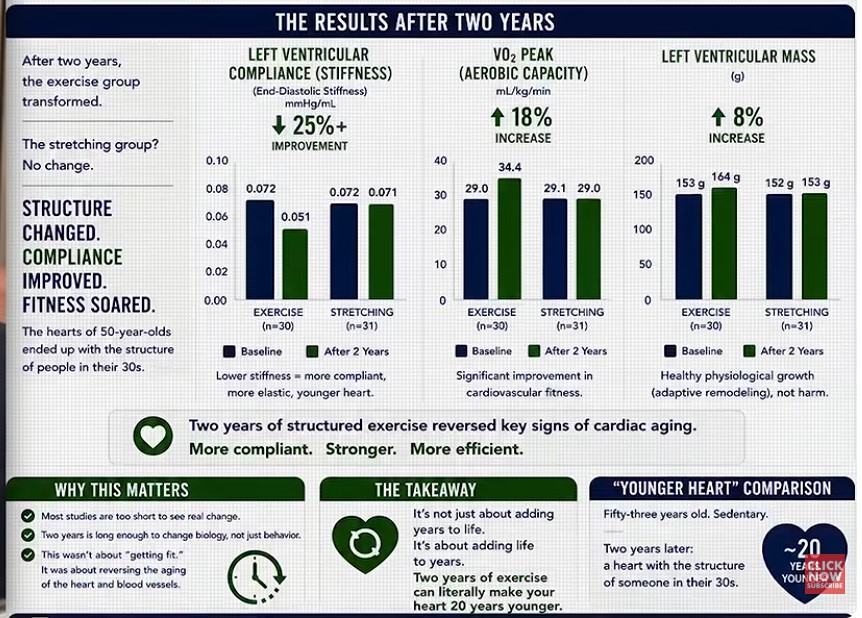
Scientists Discovered the Workout That Makes Your Heart 20 Years Younger
The Empire Strikes Back
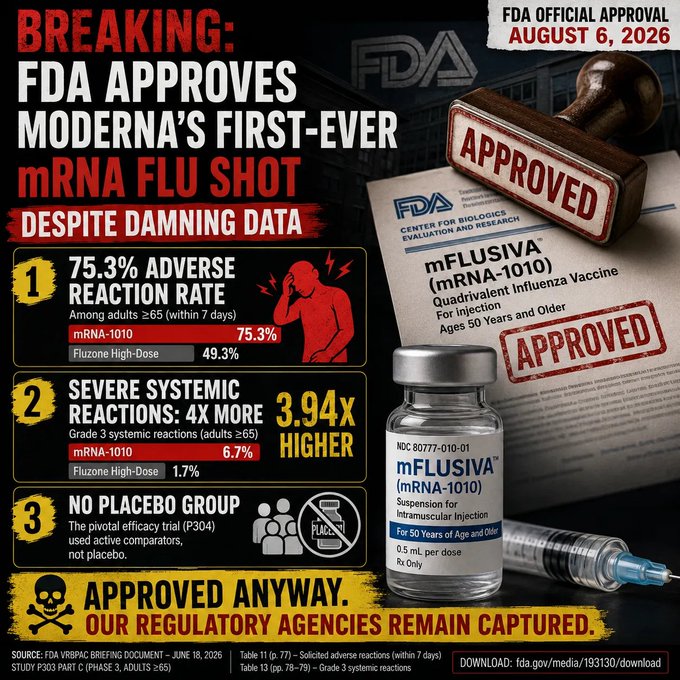
Pharma finished recapturing the Food & Drug Administration as the FDA okayed Moderna’s mRNA flu jab, which Moderna’s OWN studies show causes 270 severe side effects to stop ONE flu hospitalization.
Drug industry reform dies in darkness.
Last night, the Food & Drug Administration quietly approved Moderna’s mRNA flu “vaccine.” Moderna put out its press release at 10:15 p.m. Eastern, presumably in an effort to contain the blowback the FDA will face from MAHA and drug industry skeptics over its decision to roll over and approve this jab. Of course, legacy media outlets were ready with stories; no doubt they were tipped in advance and had pieces waiting.
As I wrote in May, the risk-benefit ratio of the jab is almost absurdly bad, based on Moderna’s own studies — which likely understate it, since drug companies will do everything they can not to connect the side effects they see in clinical trials. To quote that piece (which you can read fully below):
In other words, Moderna’s own data show that about 270 people will suffer severe vaccine side effects from its shot to stop a single flu hospitalization. In what world does that risk ratio make sense?
In a world where Moderna and Blackstone have a direct line to the White House. There was no chance the FDA would say no to this jab once the Trump Administration forced Dr. Vinay Prasad to resign from the agency in March.
The only question is whether Moderna will be able to bribe offer completely legal financial incentives to enough pharmacy benefit managers to get this new jab — which will no doubt cost far more than traditional flu shots — into the system and the arms of unwitting patients.
I’m sure benefits managers will stand up for patients and say no to a more expensive drug with worse side effects even if Moderna kicks back mucho dinero —
I’m sorry, I was laughing too hard to finish that last sentence.
Another great day for American medicine!
https://alexberenson.substack.com/p/the-moderna-flu-jab-has-a-comically
The Blue-Collar Path by Adam Sharp
Today’s college graduates are being ejected into the real world and finding a cold, harsh reality.
The job market stinks.
New York Fed data shows that 42% of recent college grads are currently in a job that doesn’t require a degree.
At big tech companies, new graduates now account for just 7% of hires. That’s down more than half since 2019.
Companies across the country are hiring fewer entry-level white-collar workers. Recruiting firm Cadient recently showed that entry level job postings have fallen 73% since 2022 (the same year ChatGPT was released – coincidence?).
If companies aren’t hiring entry-level people, how are young grads supposed to get the experience needed to get more senior jobs?
It’s brutal out there. And stocks are at all-time highs! Imagine what would happen if we got a crash and recession.
The bottom rung of the white-collar career ladder is already breaking. And it’s going to get even more challenging from here.
Blame AI, Immigration, and Outsourcing
Advanced AI agents are playing a big role in this shift. Work that was previously done by new hires and interns is being handed off to ChatGPT, DeepSeek, and Claude.
As AI agents become capable of handling increasingly complex tasks, this disturbing trend will only accelerate.
Add in the massive influx of immigrant workers on visas like the H-1B, who are taking up an increasingly large share of desk jobs, and it’s an ugly situation. These workers happily accept lower pay and longer hours (I don’t really blame them. The blame lies with our politicians for letting it happen).
The idea that America needs to import tech workers from the 3rd world is so laughable I can’t believe anyone says it with a straight face. Yet politicians on both sides of the aisle do so on a regular basis.
Big tech/AI is the worst offender when it comes to hiring foreign workers over Americans. OpenAI, maker of ChatGPT, was recently fined $3.2 million for discriminating against Americans in favor of foreign workers. According to U.S. law, companies are only supposed to get green cards for workers if they can’t find an American to do the job. But OpenAI wasn’t even trying to place Americans in some jobs. They were allegedly aiming for cheap foreign labor first. This scheme is absolutely rampant in tech.
The job listings are initially hidden, so nobody applies. Then they say “gosh nobody applied for this job we hid, so we have to hire a H-1B…”
The $3.2 million settlement is a start. But if we want this situation to change, the fines need to be a lot bigger. $3.2 million is literally nothing to big tech. Boycotts could also be an interesting tool, one which will certainly come into play eventually.
Then we have old-fashioned outsourcing, where a company fires its domestic team and boots up an operation abroad, often in India. Multiple friends of mine have been laid off due to outsourcing in recent years.
Put it all together, and it’s a rough situation for white-collar workers. Especially young ones.
The Blue-Collar Option
For a long time in this country, it felt like the only route to success was getting a college degree and finding a nice desk job. It was never really true, of course. But it sure felt that way when I was a kid.
But with the rise of AI, mass immigration, and outsourcing, this idea is breaking down.
Fortunately there is another path young people can take. The trades. And it’s going to become a lot more popular going forward.
My 17-year old son is a good example. He recently started working as an electrical apprentice. He’s already making $24 an hour. Not bad.
His senior year of high school will be spent learning the trade, while getting paid for it. It’s part of an apprenticeship program run by an organization called Independent Electrical Contractors (IEC). He’ll still graduate with his class, and even get college credits should he ever choose to pursue a degree.
IEC matched him with a local electrical company, which hired him. The company pays for his required classes, gives him a full set of tools, and offers on-the-job training. Not a bad deal.
By 21 years old, he should be making $65,000+ as a licensed journeyman electrician. And by then he should be able to save up $100,000+ living at home.
Apprenticeship programs like this are available all over the country. Many people just aren’t aware of them. For thousands of years, apprenticeships were the standard for professions. They will be again.
Blue-collar careers certainly have their advantages. No college debt, no uncertainty about AI disruption, and plenty of demand.
There are drawbacks, too, of course. It’s a physically strenuous job. But if I were his age, I’d be doing the exact same thing. I couldn’t be prouder of the path he chose.
To be clear, there are some occupations which still require a university degree. Engineering, architecture, medicine, computer science, math, etc. But AI is already eating into these jobs, and there are major disruptions on the horizon.
Let’s face it. The value of most college degrees is plummeting. Especially liberal arts. The snowball’s rolling down the hill, gathering mass and speed.
Blue-collar pay will hold up far better than most “knowledge” jobs over the next few decades. The introduction of AI practically guarantees it, even before factoring in immigration and outsourcing.
Yet despite all the emerging evidence, far too many kids still believe they need to go to college to make a decent living. This simply isn’t the case today. And it definitely won’t be in the future.
More young people should consider a career in the trades. Plumbers, electricians, welders, and other skilled workers make good money and have a lot more job security than most desk workers.
In an era filled with immigration, AI disruption, and outsourcing, the outlook for skilled blue collar work is bright.
So if there are young people in your life who are struggling with direction, encourage them to consider the trades. I’m convinced it’s the best option for many kids (and adults) today.
All the best,
Adam Sharp
for The Daily Reckoning
feedback@dailyreckoning.com