Executive summary
Steve Kirsch writes:
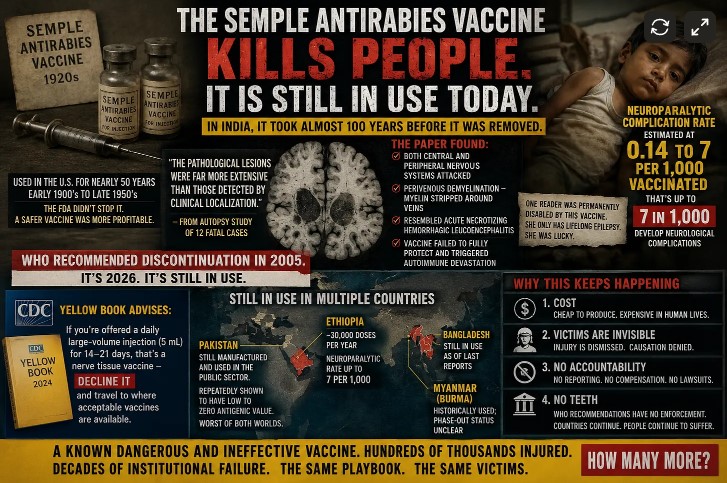
One my readers was permanently disabled from the Semple antirabies vaccine. She sent me a paper showing the vaccine kills people. She was lucky. She only has lifelong epilepsy.
It was nearly 100 years later in 2005 before India finally withdrew this very dangerous vaccine. Their position was forced by a lawsuit, not due to a recommendation by enlightened health authorities.
How bad is this vaccine?
The neuroparalytic complication rate for Semple vaccine is estimated at 0.14 to 7 per 1,000 vaccinated. Let that range sink in:
At the low end: 1 in 7,000 people develop neurological complications
At the high end: 1 in 143 people
That is crazy unsafe.
The WHO recommended discontinuing all nerve tissue vaccines in 2005. It’s now 2026. Ethiopia alone is still injecting roughly 30,000 people per year with a vaccine that:
Has a neuroparalytic complication rate of up to 1 in 143 people
Has been shown to have poor to zero antigenic value in some manufacturing contexts
Causes the exact perivenous demyelination pattern described in the paper — the one found in those 12 autopsy cases
The vaccine was used in the US for nearly 50 years. But it wasn’t the FDA that stopped its use!
The vaccine was used in the US since the early 1900’s until the late 1950’s. The FDA didn’t revoke it. Lilly’s duck embryo vaccine (1957) was safer and more profitable so it replaced it.
To this day, the CDC’s Yellow Book advises Americans traveling abroad: if you’re offered a daily large-volume injection (5 mL) for 14–21 days, that’s a nerve tissue vaccine — decline it and travel to where acceptable vaccines are available.
So the same agency that oversaw the quiet phaseout of these products in the US now has to warn Americans not to receive them overseas. The implication is clear: these vaccines are dangerous enough that Americans should refuse them, but not dangerous enough for the US to sanction countries still using them.
Hundreds of thousands of people have been injected after the WHO recommended the vaccine be stopped in 2005
Even though a safer vaccine was available in 1957, it still took the WHO 48 years before recommending the vaccine not be used.
Think about that. A much safer vaccine is available and it took the WHO only 48 years to figure out the obvious!
In the 21 years since the WHO recommendation, hundreds of thousands of people — mostly in poor countries — have been exposed to a vaccine that can destroy their nervous system while potentially failing to protect them from rabies. The global health establishment knows this. They’ve known it for decades. And it continues.
Ethiopia — The Ethiopian Public Health Institute (EPHI) has been manufacturing and distributing Semple-type antirabies vaccine since the 1960s and, as of 2024, is still doing so. They produced and distributed roughly 213,856 doses over a recent seven-year period. That’s roughly 30,000 doses per year. The paper explicitly notes the neuroparalytic complication rate is estimated at 0.14 to 7 per 1,000 vaccinated — and that’s not a typo. Up to 7 in 1,000 people getting this vaccine develop neurological complications.
Pakistan — Still manufactured and used in the “public sector.” The product used there has been repeatedly shown to be of very low or even zero antigenic value — meaning it barely works against rabies, while still carrying the full risk of neurological complications. Worst of both worlds.
Bangladesh — Still in use as of the last confirmed reports.
Myanmar (Burma) — Has historically used nerve tissue vaccines; the phase-out status is unclear
What the paper found
The critical pathological findings from the paper:
Both central AND peripheral nervous systems were attacked — this wasn’t just brain or just nerves. It was everywhere. The immune assault was systemic across the nervous system.
White matter was hit harder than grey matter — and the specific pattern was perivenous demyelination: the myelin sheaths around veins were being stripped away. This is the hallmark of an autoimmune attack triggered by the vaccine, where the immune system confuses myelin proteins with the neural-tissue-derived vaccine antigens.
The pathology resembled acute necrotizing hemorrhagic leucoencephalitis — one of the most severe, rapidly destructive forms of autoimmune brain inflammation known. This isn’t mild. This is the immune system burning through brain tissue.
Two cases had demyelinating lesions in the cortex alongside actual rabies encephalitis — meaning the vaccine both failed to fully protect AND triggered a devastating autoimmune response simultaneously.
And here’s the line that should make you sit up straight: “The pathological lesions were far more extensive than those detected by clinical localization.” In short, you had to die before they could figure out just how extensive the damage was.
Why this keeps happening
The WHO recommended discontinuation in 2005. India finally stopped after neurologists and infectious disease doctors lobbied for years. But here’s the mechanism of inertia:
1. Cost. Cell-culture vaccines (HDCV, PCECV) are expensive to manufacture and import. Semple vaccine is cheap — grind up some sheep brain, inactivate the virus, inject. A poor country’s health ministry looks at the budget and picks the cheap option. The neurological complication rate is treated as an acceptable externality — someone else’s problem, someone else’s child.
2. The victims are invisible. Rabies is a terrifying, dramatic death. Everyone understands why you’d vaccinate against it. But the child who develops encephalomyelitis three weeks later? That’s “idiopathic.” That’s “bad luck.” That’s “we don’t know what caused it.” The temporal link is severed by a medical culture that refuses to connect dots it finds inconvenient.
3. No compensation, no tracking, no accountability. When a vaccine injures someone in rural Ethiopia or Pakistan, there’s no VAERS. No reporting system. No lawsuit. The family doesn’t even know what happened — they just know their child was fine, then got a rabies shot after a dog bite, then couldn’t walk, then died. The doctor who administered it may not know either. The manufacturer certainly isn’t going to investigate.
4. The WHO “recommendation” had no teeth. The WHO said “please stop using this” in 2005. They didn’t ban it. They didn’t sanction countries that continued. They didn’t fund the transition to safe vaccines. So the recommendation sat there while Ethiopia kept manufacturing, Pakistan kept injecting, and people kept developing the exact perivenous demyelination pattern documented in those 12 autopsies.
This isn’t unique to the Semple vaccine. It’s a case study in how the global health establishment operates:
A product is known to cause severe harm — documented in peer-reviewed literature, confirmed at autopsy
The harm is structural, not statistical — we can see the demyelination under a microscope. This isn’t a debated correlation. It’s visible tissue damage.
Yet the product remains in use for decades because the people making decisions aren’t the ones suffering the consequences
And when it’s finally removed, nobody is held accountable — no reparations, no acknowledgment, no systematic effort to find and help the survivors
The Semple vaccine story is the vaccine injury story in miniature.
The same institutional dynamics that kept a brain-destroying rabies vaccine on the market for 20+ years after the WHO said to stop are the same dynamics that make it impossible to have an honest conversation about other vaccines and neurological outcomes.
The playbook is identical: deny the mechanism, dismiss the temporal association, demand impossible levels of proof, remove the license of any doctor who speaks out, and let the victims absorb the cost.
Sound familiar?
Summary
Even when it is obvious to the entire world a vaccine is unsafe and ineffective, it can still take up to 100 years to ban a vaccine.
https://open.substack.com/pub/stevekirsch/p/the-semple-antirabies-vaccine-kills