While we still live in an insane society where others cannot be trusted it behooves us to be able to protect ourselves, our families and friends. To prevent us from being able to do that is tyrannical oppression.

Tom's Blog on Life and Livingness
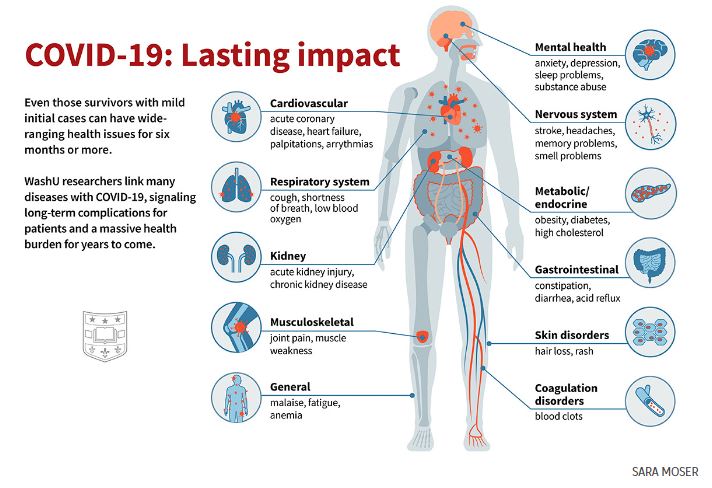
Among COVID-19 survivors, an increased risk of death, serious illness
https://medicine.washu.edu/news/among-covid-19-survivors-an-increased-risk-of-death-serious-illness/
I recently saw a report of a study that found 70% of long Covid sufferers had never had Covid, they had only received the jab.
To aid those tricked/coerced into getting the jab as well as those suffering from symptoms of shedding after being exposed to the jabbed, I have done my best to compile a Jab Recovery Protocol from the various sources I have seen: https://www.tomgrimshaw.com/tomsblog/?p=35644
And this is my attempt to assist those who don’t feel up to sourcing and compiling the ingredients themselves:
https://www.healthelicious.com.au/NutriBlast-Anti-Spike.html

We know that excess carbs like sugar and white flour can make us gain weight, but there are other culprits lurking in the food supply.
Recently the Washington Post published a puff piece on monosodium glutamate (MSG), claiming that we have nothing to fear from the artificial flavoring that adds umami “spark” to many dishes. The author, Aaron Hutchinson, marginalizes headaches and allergic reactions as minor symptom in a few hypersensitive people. Says Hutchinson:
“In addition to soup and eggs, MSG can be added to salad dressings, bread, tomato sauce, meats, popcorn, ‘an absolutely filthy martini,’ you name it. MSG is a great way to add flavor to just about anything except sweets. It’s particularly great with vegetables, too.”
He makes no mention of the real problem with MSG: weight gain. If you search “msg-induced obesity” at PubMed, you will come up with almost one hundred citations. It’s hard to get research animals to overeat and become obese — in order to study obesity — so scientists feed the rats, mice and hamsters MSG to make them eat more and put on weight.
Most of the citations are animal studies, not human trials, and the food industry has argued that the amount of MSG given to the animals is way more, as a function of body weight, than humans would ever eat. Or, they say, the association with weight gain and MSG is really an association of weight gain and processed foods, since MSG is in almost all processed foods.
What happens when we consume small amounts of MSG as a flavoring day after day after day? A 2008 study1 published in the journal Obesity provides confirmation that MSG indeed causes weight gain in humans, and not because of its inclusion in processed foods.
In this well-designed trial, researchers at the University of North Carolina at Chapel Hill studied 750 Chinese men and women, ages 40-59, living in three rural Chinese villages. Most of the study subjects prepared their meals at home without commercial processed foods and about 82% used MSG.
Those participants who used the highest amounts of MSG had nearly three times the incidence of overweight as those who did not use MSG, even when physical activity and caloric intake were accounted for.
What about the argument that the glutamic acid in MSG is the same as the essential amino acid glutamic acid that we get from protein foods? According to the Washington Post article, “The glutamate in MSG is chemically indistinguishable from glutamate present in food proteins. Our bodies ultimately metabolize both sources of glutamate in the same way.” The first sentence is true but the second sentence is false.
The glutamic acid in foods like meat is attached to various peptides and other compounds that release it when required and prevent it from overstimulating the nervous and endocrine systems; while the glutamic acid in MSG is “naked,” highly reactive and unmitigated by its milieu.
Americans consumed about one million pounds of MSG in 1950; today that number is three-hundred million pounds. Almost all processed and fast food contains MSG2 (usually not labeled), and the food industry certainly knows that the additive they use to make their food taste good is a major cause of the current obesity epidemic. The message to consumers is clear: to lose weight, it’s important to avoid all processed food, and certainly not add it to the foods you prepare at home.
As I have never met a diet soda-drinker who is slim, the results of a review study by Susie Swithers, Purdue University professor of psychological sciences and a behavioral neuroscientist, do not surprise me. Swithers found that consumption of diet soft drinks increases the likelihood of overeating.
One large study found that people who drink artificially sweetened sodas are more likely to experience weight gain than those who drink non-diet sodas. Other studies3 found that those who drink diet sodas have twice the risk of developing metabolic syndrome, often a precursor to cardiovascular disease, than those who abstained.
Use of diet sodas, sweetened with non-caloric sweeteners such as aspartame, sucralose and saccharin, has increased enormously over the last twenty-five years, as consumers try to steer clear of sugar and high fructose corn syrup. About 30% of American adults regularly consume these artificial sweeteners. What to drink if you need to watch your weight?
Try sour kombucha made with organic cane sugar — look for kombucha with less than 5 grams of sugar per serving. Or, make your own, letting it brew a long time (see my blog post “Kombucha Like Fine Champagne”4). Sparkling water with a squeeze of lemon and pinch of unrefined salt makes a refreshing and healthy soft drink. Herbal tea and bone broth are additional choices.
When it comes to weight loss, not all fats and oils are the same. Many studies have shown that saturated animal fats are far less likely to cause weight gain than polyunsaturated vegetable oils.
For example, one study5 found that mice fed excessive corn oil had increased caloric intake and obesity. In another,6 rats were divided into different groups receiving diets with identical proportions of calories from fat, protein, and carbohydrate but different types of fats.
The rats in the group receiving fat from safflower oil had a 12.3% increase in total body weight compared to the rats eating traditional fats. Weight gain was lower in the rats fed a higher proportion of saturated fats. For the average human, a 12.3% increase in total body weight translates into 23 pounds.
Vegetable oils that have been heated are even more obesogenic. In a randomized trial on rabbits,7 three groups of rabbits were given access to identical foods, with only one difference: the first group of rabbits was fed unheated vegetable oil, the second group was fed vegetable oil that had been heated once, and the third group was fed vegetable oil that had been repeatedly heated multiple times — as happens in deep friers. Everything else about their diets was kept the same.
The surprising outcome was that compared to the group of rabbits eating unheated oil, the group eating single heated oil gained 6% more weight, and the group eating repeatedly heated oil gained 45% more weight — even though the rabbits eating heated oil actually consumed a slightly lower level of calories. It seems that foods fried in vegetable oil are dieters’ worst enemy. Why would polyunsaturated vegetable oils cause weight gain? As explained by Jeff Nobbs:8
“When we eat a diet high in polyunsaturated fatty acids, omega-6s and or linoleic acid, over time, this leads to mitochondrial dysfunction, primarily with our electron transport chain. And the ETC is a very important process that creates ATP or energy … if these processes become dysfunctional, this is really bad, because what happens is we can’t effectively or properly burn fat as fuel.
Another thing that we start to see is reduced fatty acid beta oxidation which also means that we become less efficient at using fat as fuel and as a result we begin to prioritize carbohydrates as fuel … we are consuming high amounts of vegetable oils, we become less efficient at using fat as energy, while also making our fat cells bigger and grow in size, which is exactly what we don’t want and this could be a huge reason why we’re gaining weight and why it’s so difficult for us to lose weight!”
Dieters are often reluctant to embrace saturated animal fats, believing the propaganda that butter and lard will make you fat. But the science suggests otherwise. For example, a study9 by Temple University School of Medicine provides welcome vindication for Atkins and other practitioners who insist that the best way to lose weight is to eat a lot of fat — animal fat.
The study took place in a clinical research center where every calorie eaten and spent was measured. After a week of typical eating, 10 obese patients with Type 2 diabetes followed a diet that limited carbohydrates to 20 grams per day but allowed unlimited protein and fat.
With carbs out of the diet, the patients spontaneously reduced their daily energy consumption by 1,000 calories per day. “When carbohydrates were restricted,” said lead researcher Guenther Boden, MD, “the subjects spontaneously reduced their caloric intake to a level appropriate for their height, did not compensate by eating more protein or fat, and lost weight. We concluded that excessive overeating had been fueled by carbohydrates.”
In addition to calorie reduction and weight loss, subjects experienced markedly improved glucose levels and insulin sensitivity as well as lower triglycerides and cholesterol. The interesting thing about this study was that the subjects did not consciously try to restrict calories or lose weight, showing that restricting carbs and increasing fat in the diet works better than will power.
In yet another defeat for the low fat, you-must-suffer-to-lose-weight school of thought, a Swedish study10 has found that women who regularly consume at least one serving of full-fat dairy every day gained about 30% less weight than women who didn’t.
The researchers, from the Karolinska Institute in Stockholm, looked at the intake of whole, sour, medium- and low-fat milk, as well as cheese and butter for almost twenty-thousand Swedish women aged 40-55 years old — the age when most women should and do gain weight … but not too much.
The researchers reported that a regular and constant intake of whole milk, sour milk and cheese was significantly and inversely associated with weight gain (that is, those consuming whole-milk products did not gain much weight), compared to the other groups.
A constant intake of at least one daily serving of whole and sour milk was associated with 15% less weight gain, while cheese was associated with 30% less weight gain.
Two other studies have concluded that the consumption of whole fat dairy products is linked to reduced body fat. In one paper,11 middle aged men who consumed high-fat milk, butter and cream were significantly less likely to become obese over a period of 12 years compared to men who never or rarely ate high-fat dairy.
The second study12 is a meta-analysis of sixteen observational studies aimed at exploring the hypothesis that high-fat dairy foods contribute to obesity and heart disease risk. The researchers concluded that the evidence does not support this hypothesis; in fact, the reviewers found that in most of the studies, high-fat dairy consumption was associated with a lower risk of obesity.
The tragic practice of feeding reduced-fat milk to growing children, even prohibiting full-fat milk in schools and day care centers, in order to prevent weight gain, has no basis in science, as shown in a study13 from Canada.
Researchers followed over 2,700 children, ages 1 to 6. Children who got full-fat milk had a lower body mass index and also higher vitamin D status. Children who drank full-fat milk were less likely to end up hungry, and less likely to snack on high-calorie foods, suggested the researchers.
In U.S. schools, children have a choice of low-fat milk, which they hate, or chocolate milk made with skim milk powder and high fructose corn syrup — often containing almost as much sweetener as sodas! The message is clear: for weight loss, avoid all industrial seed oils and enjoy animal fats and full-fat dairy foods.
When you eat too much salt, you become thirsty and drink water so as to dilute the amount of sodium chloride in the bloodstream, keeping sodium at the proper levels and excreting the excess. This is the conventional view of the “salt equation.”
But experiments with mice found that mice burned more calories when they got more salt, eating 25% more just to maintain their weight. It seems that salt stimulates the production of more glucocorticoid hormones, which break down fat and muscle in the body.
In addition, salt-detecting neurons in the mouth control the urge to drink, and more salt results in a lower sensation of thirst. “The work suggests that we really do not understand the effect of sodium chloride on the body,” said a study author.14 “These effects may be far more complex and far-reaching than the relatively simple laws that dictate movement of fluid, based on pressures and particles.”
These results suggest that increasing salt may be a useful strategy for weight loss, as long as the diet contains sufficient levels of fat to mitigate increased feelings of hunger. The results also show the folly of the recent FDA push15 to get the food industry to lower salt content in processed foods.
The food industry isn’t complaining because they now have an additive they can use to make low-salt foods taste saltier: it’s called Senomyx. Senomyx and other flavor enhancers stimulate your taste buds without them actually tasting anything. Much like MSG, these flavor enhancers operate on the neurological level to produce these reactions.
Since they are not actually ingredients but rather “enhancers,” FDA does not require manufacturers to list them in the ingredients panel except as “artificial flavors.” Because very small amounts of the additives are used, Senomyx’s chemicals have not undergone the FDA’s usual safety approval process for food additives.
In fact, they are not flavors at all. They are chemicals that contain no flavor of their own, rather they activate or block taste receptors in your mouth. The chemicals can mimic or enhance the taste not only of salt, but also sugar and monosodium glutamate (MSG).
Already the industry is adding Senomyx to a huge number of products, from soups to coffee (for a salty taste) and from sodas to candies (for a sweet taste).16 So what could possibly go wrong?
Here’s one thing: your body has an absolute requirement for salt and if we don’t get the salt we need in our food, we just might eat and eat and eat salty-tasting foods in order to get the salt we need. Sounds like a great recipe for weight gain.
Those who write about the worldwide obesity epidemic have focused almost exclusively on life style issues such as consumption of high-calorie junk food and decreases in exercise. These remain plausible interpretations and are certainly contributing factors.
But new research opens up an entirely new theory — the disruption of weight regulation by hormone-disrupting contaminants. Japanese researchers17 have found that exposure to bisphenol A (BPA) in combination with insulin increases the number of fat cells in mouse cell tissue culture, and also causes the enlargement of fat cells.
Human exposure is widespread through consumption of water in plastic bottles. (Other sources are dental sealants, used on children’s teeth to “prevent cavities,” and foods packaged in plastic.)
Dr. Barry Durrant-Peatfield of the UK has also proposed the theory that even drinking water from the tap can make you fat — fluoridated water, that is. “There is no doubt that fluoride is enzyme disruptive and one thing it affects is thyroid hormones. As a result of this disruption, people can finish up with partial under-activity of the thyroid gland.”
According to Dr. Durrant-Peatfield, fluorine can replace iodine in the body, leading to thyroid problems and weight gain. He believes that children may be particularly susceptible to obesity if their mothers drank fluoridated water while pregnant.
He notes that UK obesity levels are highest in the West Midlands, the only area in England now fluoridated (Sunday Mercury, July 11, 2004). Yes, lots of compounds that make us gain weight are lurking in the food supply! If you want to lose weight, the very first assignment is to avoid them like the plague.
Sally Fallon Morell is author of the best-selling cookbook Nourishing Traditions and many other books on diet and health. She is the founding president of the Weston A. Price Foundation (westonaprice.org) and a founder of A Campaign for Real Milk (realmilk.com). Visit her blog at nourishingtraditions.com.
Article copied from Dr Joseph Mercola web site.
Mark Farnell writes: Feeling sad at the news of a friend and fellow researcher’s unexpected death (I reckon they bumped her off tbh, her exposes were that good). In honour of Tracey, I can do no better than plug her last book- it’s a fantastic read. Her memory will live on in her work.

You may have heard about how bad vegetable oils are by now. But have you ever wondered why? My biggest beef with vegetable oils is that they negatively impact your metabolic rate and gut health — the two most important factors that impact your state of health.
So, yah. It’s kind of a big deal that our food system is centered around them. And that mainstream nutrition advice from Harvard still recommends vegetable oil as a “healthy fat” because it lowers serum cholesterol.
But what about the well-known fact that PUFAs (polyunsaturated fats) are very unstable molecules? (And vegetable oils are high in PUFAs, specifically linoleic acid, an omega-6).
“Polyunsaturated fatty acids (PUFAs) are highly susceptible to lipid per oxidation because of their unstable double bonds.1
PUFAs, in this sense, are like delicate glass … When glass shatters, it invariably leaves behind a mess of dangerous shards … Likewise, when PUFAs shatter they leave behind shards such as MDA, which are capable of damaging proteins, DNA and other structurally and functionally important components of our cells.” ~ Chris Masterjohn, Ph.D.2
Having more of these fats around creates a damaging internal environment in your body. Thus, there are long term negative health consequences with high PUFA consumption. Let’s discuss a few of these consequences.
First, vegetable oils wreak havoc on the gut by increasing tight junction permeability.3 Tight junctions play an important role in intestinal barrier function by maintaining selective permeability. Well, unfortunately, PUFAs can increase the permeability of tight junctions. (Not what we want!)
In one study, the omega-6 PUFA rich diet increased host inflammation, oxidative stress, and gut barrier dysfunction:4
“The corn oil diet, rich in omega-6 polyunsaturated fatty acids, increased the potential for pathobiont survival and invasion in an inflamed, oxidized and damaged gut while saturated fatty acids promoted compensatory inflammatory responses involved in tissue healing.
We conclude that various lipids uniquely alter the host-microbe interaction in the gut. While high-fat consumption has a distinct impact on the gut microbiota, the type of fatty acids alters the relative microbial abundances and predicted functions. These results support that the type of fat are key to understanding the biological effects of high-fat diets on gut health.”
Okay so I will just up my omega-3s, the healthy PUFAs, right? Ehh, not so fast. High dietary omega-6 PUFA consumption has been shown to shift the gut microbiome and can induce gut dysbiosis and inflammation.5
But the authors of this study point out that while omega-3 PUFAs may lead to short-term inflammation reduction, this was due to immune suppression, which eventually led to other health problems and increased mortality.
Saturated fats are stable molecules and are protective. Unsaturated fats are unstable and can cause a lot of damage when consumed in excess. So, it makes sense why the gut can be damaged in the long run with high PUFA consumption.
“Clinically, excessive ω-6 polyunsaturated fatty acid (PUFA) and inadequate ω-3 PUFA have been associated with enhanced risks for developing ulcerative colitis. In rodent models, ω-3 PUFAs have been shown to either attenuate or exacerbate colitis in different studies.
We hypothesized that a high ω-6: ω-3 PUFA ratio would increase colitis susceptibility through the microbe-immunity nexus. To address this, we fed post-weaned mice diets rich in ω-6 PUFA (corn oil) and diets supplemented with ω-3 PUFA (corn oil + fish oil) for 5 weeks. We evaluated the intestinal microbiota, induced colitis with Citrobacter rodentium and followed disease progression.
We found that ω-6 PUFA enriched the microbiota with Enterobacteriaceae, Segmented Filamentous Bacteria and Clostridia spp., all known to induce inflammation. During infection-induced colitis, ω-6 PUFA fed mice had exacerbated intestinal damage, immune cell infiltration, prostaglandin E2 expression and C. rodentium translocation across the intestinal mucosae.
Addition of ω-3 PUFA on a high ω-6 PUFA diet, reversed inflammatory-inducing microbial blooms and enriched beneficial microbes like Lactobacillus and Bifidobacteria, reduced immune cell infiltration and impaired cytokine/chemokine induction during infection.
While, ω-3 PUFA supplementation protected against severe colitis, these mice suffered greater mortality associated with sepsis-related serum factors such as LPS binding protein, IL-15 and TNF-α. These mice also demonstrated decreased expression of intestinal alkaline phosphatase and an inability to dephosphorylate LPS.
Thus, the colonic microbiota is altered differentially through varying PUFA composition, conferring altered susceptibility to colitis. Overall, ω-6 PUFA enriches pro-inflammatory microbes and augments colitis; but prevents infection-induced systemic inflammation.
In contrast, ω-3 PUFA supplementation reverses the effects of the ω-6 PUFA diet but impairs infection-induced responses resulting in sepsis. We conclude that as an anti-inflammatory agent, ω-3 PUFA supplementation during infection may prove detrimental when host inflammatory responses are critical for survival.”6
PUFAs Negatively Impact Thyroid and Metabolic Health
Another consequence of high PUFA consumption is that PUFAs can negatively impact thyroid and metabolic health since they interfere with your cell’s ability to utilize active thyroid hormone. It’s great that our body can convert T4 to active T3. But to increase energy production, our cells must be able to access that T3.
In fact, tissue T3 levels are different than serum T3,7 which is why one of the best ways to assess metabolic and thyroid health is through body temperature and pulse measurements (which I discuss in depth here), since higher cellular T3 increases the metabolic rate, raises body temperature, and increases our pulse.8 Understanding this helps us realize why it’s a bad thing that PUFAs interfere with your cell’s ability to use active thyroid hormone, T3.
“Safflower oil [high in Omega-6 PUFA] was more effective than tallow as a repressor of T3 action … polyunsaturated fats uniquely suppress the gene expression of lipogenic enzymes by functioning as competitive inhibitors of T3 action, possibly at the nuclear receptor level.9
The potency of unsaturated fatty acids for INB (Inhibition of Nuclear T3 Binding) was greater than of saturated fatty acids, and increased with the number of double bonds.10
The effects of selected fatty acids (linoleic – PUFA, oleic – MUFA, and palmitic – SFA) on triiodothyronine (T3)-receptor binding were compared … the rank order of potency for inhibition was linoleic acid greater than oleic acid greater than palmitic acid.”11
It’s never about extremes. You cannot eat a zero PUFA diet and that is not the goal. But you do not need to over consume PUFAs. You do not need to add more omega-3s to your diet if you are consuming animal fats. You do not need to add fish oils, you do not need to force flax seeds down your throat. And you certainly don’t need to increase your vegetable oil consumption.
Instead, eat real, whole foods. And for your fats, prioritize animal fats that are rich in the stable, protective saturated fats. Just like your great grandma. This will provide your body with more of an optimal fatty acid profile without over thinking it. Plus, this approach just makes sense.
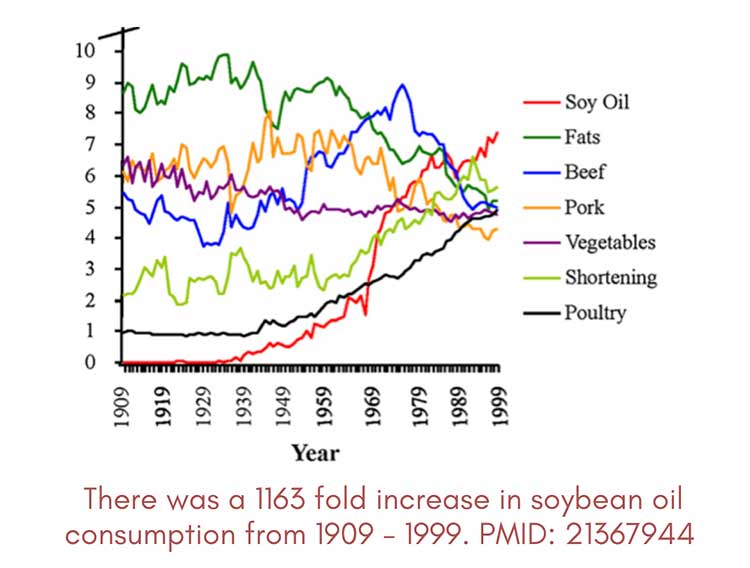
Vegetable oils did not exist 100 years ago. People did not force fish oils down their throat. They enjoyed a diet rich in animal products, and consumed saturated fat without fear. And the rates of autoimmune and chronic diseases we face today was certainly not as high.
What your food eats, matters — as pigs and chickens are vehicles for vegetable oils. (So if their diet is high in PUFAs, the final product will contain more PUFAs). With the current agriculture system, knowing where your food comes from is vital. The article was written by Ashley Armstrong, who is passionate about providing the highest quality food possible.
Armstrong is the cofounder of Angel Acres Egg Co., which specializes in low-PUFA (polyunsaturated fat) eggs. We discussed the importance of low-PUFA eggs in a recent interview, embedded above for your convenience.
Angel Acres Egg Co. ships Low PUFA eggs to all 50 states — but there is currently a waiting list as she slowly increases the number of chickens within the network to fulfill the demand. More egg boxes will be available this spring — join the waitlist for low PUFA egg boxes here.
Armstrong also co-founded Nourish Cooperative which ships the best low PUFA pork, beef, cheese & A2 dairy and traditional sourdough to all 50 states. They are also close to accepting new members to the farm cooperative — join the waitlist here: nourishcooperative.com.
In the video segment above Ashley reflects on the timeline of her decision to invest her free time into regenerative farming. Considering how just a few years ago, her health was far from ideal. She struggled with mitochondrial energy production, and her body was in a low thyroid state. Your body prioritizes energy for essential tasks, and decision-making requires significant energy.
Your brain consumes about 20% of your body’s energy despite being only 2% of its weight. Ashley simply would not have had enough cellular energy to supply her brain to make a decision like she did unless she improved her health. Factors like excess linoleic acid, estrogen and endotoxins were depleting her cellular energy, which is crucial for making energy-intensive decisions.
Her transformation underscores the power of nurturing your health to gain the energy necessary for making significant life changes. Avoiding dietary pitfalls like seed oils played a key role in this journey, enabling her to tap into a newfound capacity for brave decisions — a testament to the profound impact of regaining cellular energy on her ability to navigate life’s choices.
It is my sincere desire and hope that you consider her journey to inspire and empower you to make similar choices in your own life and reclaim the Joy that you deserve. Imagine experiencing the nearly limitless Joy that Ashley has with her 1,000 chickens and four Livestock Guard Dogs below.
From Dr Joseph Mercola:
https://articles.mercola.com/sites/articles/archive/2024/03/11/vegetable-oils-wreck-your-gut.aspx

Yet another example of the principle that if you do the opposite of what the main stream media promote and believe the opposite of what they say then you are going to be right a lot more often than wrong.
In this interview, Christy Sutton, D.C., reviews the dangers of excessive iron. While most doctors look for iron deficiency, few ever pay attention to elevated iron. Sutton is the author of two books, “Genetic Testing: Defining Your Path to a Personalized Health Plan: An Integrative Approach to Optimize Health,” and “The Iron Curse, Is Your Doctor Letting High Iron Destroy Your Health?”
Iron plays an important role in health, especially for children and young adults. Without sufficient iron, you’re not going to be able to form red blood cells and certain proteins in your mitochondria that are responsible for producing energy. On the flip-side, an excess of iron can cause significant damage.
Sutton’s interest in iron has been “lifelong” she says, as she struggled with low iron while her husband has a genetic anomaly that causes him to have elevated iron levels. So, she has personal experience with both ends of the spectrum.
“I have Crohn’s [disease], celiac, and lost part of my small intestine due to Crohn’s when I was 16,” she says. “Because of that, I have to take a bile sequestrant. Then, being menstruating female who’s had a child, low iron has been something that I have been watched very closely for and I had to take iron a lot.
Like a lot of clinicians, when I came into practice, I seemed to be more hyper-focused on people’s problems that were my own problems. I dealt with iron issues. So, I wanted to watch my patients’ iron levels closely. Then I realized, ‘Oh, not everybody is low. A lot of people actually have high iron.’
It wasn’t until I was writing my first book, ‘Genetic Testing: Defining Your Path to a Personalized Health Plan,’ that I discovered the hemochromatosis genes. I realized that my husband had a hemochromatosis gene, and I realized that that was why I kept telling him to donate blood.
His doctor would order iron labs, ferritin, CBC, and he would get elevated iron often, high ferritin. He was developing high liver enzymes and his red blood cells were getting high as well, which is a common issue with people that have too much iron …
He went to a gastroenterologist, because he was trying to figure out why his liver enzymes were high. I thought it was the high iron, but that was presented to the gastroenterologist and dismissed. So, they went down this rabbit hole of misdiagnosing him with autoimmune hepatitis.
Later we went to a hematologist where we figured out he had hereditary hemochromatosis. So, it’s not something that’s particularly difficult to treat. Removing blood, diet supplements, things like that can help.
But once I got really savvy about looking for the genes and the labs combined, I realized that this is a silent epidemic that is not really being talked about. I would tell people, ‘You have a problem with high iron,’ and then they would often go and get a second opinion.
Their second opinion would say, ‘You’re fine. Don’t worry about it,’ which is a common issue where people are getting high iron labs that should warrant more investigation and then they’re just getting dismissed.”
I have beta thalassemia, a hemolytic anemia that results in a high turnover of red blood cells. My red blood cells only live about two months, rather than the normal three months. As a result, my iron tends to accumulate because of the rapid turnover. So, while I do not have the hemochromatosis gene, it results in similar problems. I inherited it from my father, who had a ferritin level close to 1,000 by the time he was diagnosed. Ideally, it should be below 40.
One of the supplements he tried was inositol, also referred to as hexaphosphate or IP-6, but it did nothing. I rapidly came to the conclusion that the supplements typically recommended for high iron are useless and potentially even dangerous, because they prevent you from doing what is really helpful, which is to remove iron through regular phlebotomies.
The most effective way to lower your iron is to donate blood two to four times a year. If losing 10% of your blood in one sitting is problematic for you, then you can remove blood in smaller amounts once a month on the schedule I have listed below. If you have congestive heart failure or severe COPD, you should discuss this with your doctor, but otherwise this is a fairly appropriate recommendation for most.
| Men | Postmenopausal Women | Premenopausal Women |
|---|---|---|
| 150 ml | 100 ml | 50 ml |
As it turns out, Sutton did not include IP-6 in her book, as she couldn’t find any research to back up the claims. She doesn’t dismiss all supplements, however. One of the most helpful, in her view, is curcumin.
“Clinically, I have seen curcumin’s ability to lower iron almost to a fault,” she says. “It’s annoying to me, because I can’t take curcumin for inflammation because it makes me low in iron. But for people that are high in iron or even inflamed with high iron, high ferritin, that’s a great place to start, because curcumin binds to iron.
It also has all of these other wonderful health promoting properties. It’s so good for your brain — it actually helps remove excess iron from the brain and other organs, the heart, liver, spleen.
So, unlike other iron chelators that might be used pharmaceutically, it doesn’t have all these possible negative side effects, but it works very effectively. I mean, I’ve seen it be used in hereditary hemochromatosis patients to lower iron without blood removal … Now, people that have really high iron might need 3 grams a day, which can create diarrhea. So, you have to look at other potentially limiting factors.”
She also recommends taking curcumin with an iron-rich meal, such as shellfish or red meat, to inhibit iron uptake. Other supplements that help bind iron include silymarin, (an extract from milk thistle). It too is very good for hemochromatosis patients, because it lowers iron and helps protect and repair the liver. Another thing that binds to and lowers iron is alpha-lipoic acid. It’s also great for protecting nerves and lowering blood sugar.
“I don’t think silymarin lowers iron quite as much as curcumin, but it’s still a significant way to lower iron,” she says. “The best way to take these — to lower iron — is take them with iron-rich meals. If you want to take them just for medicinal properties but not to lower iron, take them away from iron-rich meals.”
Health Risks Associated With High Iron
The health risks of high iron are manifold and include an elevated risk of skin infections and skin cancer. I suspect high iron may actually be a catalyst when it comes to skin cancer, along with high linoleic acid (LA) intake. LA is oxidized by iron, creating something called lipofuscin, which is basically iron attached to oxidized LA.
A more common term for lipofuscin is liver spots. So, liver spots are a dermal representation of oxidative damage to LA by high iron. Similarly, skin cancer is likely driven by a combination of high LA and high iron. Ancestral LA levels were below 2%. Today, the average is around 25%. If you had normal ancestral levels, you could have higher iron yet not get as much damage.
There are several potential diagnoses related to iron, including iron deficient anemia, copper deficient anemia, iron overload and hereditary hemochromatosis, and getting to the correct diagnosis can be tricky.
“The nice thing is that you can always fall back on labs,” Sutton says. “You don’t want to just use symptoms to guide you, because if you’re using symptoms, then this person is well far down a pathological path that you could have potentially stopped years ago, if not decades before.”
Starting with hereditary hemochromatosis, this is when you have inherited one of three hemochromatosis genes, which causes increased iron absorption by decreasing hepcidin, a liver protein. If you have the hemochromatosis gene, you don’t make as much hepcidin, causing you to absorb more iron.
That can become pathological, because over time, you just keep absorbing more and more iron, until your body finally runs out of places to put it. The first place that gets overloaded is your liver. After that, your body will store the iron in other organs, such as your heart, pancreas, brain, pituitary gland, gonads, ovaries, testes and skin.
Eventually, the iron will go everywhere because the human body has evolved to hold onto as much iron as possible. The only way, really, to lose iron is through blood loss. This is why menstruating women have a lower risk for high iron and a higher risk for low iron.
“Having said that, when you start looking at the hemochromatosis genes, all bets are off, because you’ll see females that have these hemochromatosis genes that develop high iron … you will even see children with the hemochromatosis genes that develop high iron,” Sutton says.
“I discovered that in my colleague’s 5-year-old, where predatory hemochromatosis was causing her to have severe neurological problems. That was a very difficult thing to get through because the hematologist didn’t really want to deal with it.
When you look at labs, hereditary hemochromatosis can look very similar to non-hereditary hemochromatosis, which is where you have high iron but you don’t have one of those hemochromatosis genes.
So, for you, you have more of a non-hereditary secondary hemochromatosis, because you have that thalassemia issue where your red blood cells are breaking and letting all this iron out and then you develop high iron with potentially low red blood cells.
That’s common with thalassemia. Some people, they don’t have a thalassemia gene and they develop high iron without hemochromatosis gene, because they’re just eating a lot of iron-rich foods and they’re not losing iron through menstruation. This is usually men.”
When it comes to lab work, Sutton recommends starting with a full iron panel, a complete blood count (CBC) test, gamma-glutamyl transferase (GGT), and a comprehensive metabolic panel to ensure you have sufficient liver enzymes. Measuring your copper and ceruloplasmin levels can also be helpful.
“The full iron panel has the ferritin, the TIBC [total iron-binding capacity], the UIBC [unsaturated iron-binding capacity], the serum iron and the iron saturation. With hereditary hemochromatosis, you develop high ferritin with a high iron saturation. That combination is hereditary hemochromatosis. So, over 45% iron saturation and high ferritin …
With hereditary hemochromatosis, you’ll see high iron, you’ll see the TIBC go low, the UIBC go low. The serum iron often goes high, and then that ferritin will go high. You’ll often see the liver enzymes go high and it’s common to see the red blood cells, hemoglobin, hematocrit go high.
But that doesn’t always happen. These days, so many are taking testosterone. So, you have to always ask, ‘Are you on testosterone?’ Because that can cause red blood cells, hemoglobin, hematocrit to go high as well …
I always get the GGT as a part of the labs that I order. Occasionally, I will see a high GGT when the AST and ALT, which are the other two liver enzymes, are normal. More often than not, I’ll see a high ALT or high AST. Usually, if they’re not drinking alcohol and they just have high iron, you’re going to see that high ALT.”
Sutton recommends keeping ferritin below 100. Ferritin above 100 means you’re either inflamed, have high iron, or both. Studies referenced in her book suggest that anything over 200 is pathological. The higher your ferritin level, the shorter your lifespan. You’re also more likely to die of a heart attack and cancer.
“I feel like 100 is high enough that I’m not swooping everybody in, but low enough that I’m not leaving stragglers out,” she says. “Now, if somebody has a ferritin over 100 with an iron saturation that is in the 40s or higher, then I’m highly suspicious of a hemochromatosis gene and I immediately want to get those hemochromatosis genes tested.
If they have a hemochromatosis gene, then we know why they’re high on iron and we know where this story is going — and it’s not going to be a pretty picture most likely. Then it’s time to refer to a hematologist … and talk to them about how to get iron lower …
The key is, if you don’t have a hemochromatosis gene, then you need to figure out ‘Why does this person have high iron? Do they have a thalassemia gene? Are they just eating a lot of iron?’ And then, ‘Do they have hemolysis for some unknown reason?’ That’s a non-hereditary hemochromatosis situation.
The treatment is basically the same, other than you want to use more of the supplements, go really heavy on the supplements to lower iron. If you have plenty of red blood cells and hemoglobin, then therapeutic phlebotomy is a wonderful place to start.
A lot of times people don’t because they either have a thalassemia issue where their red blood cells are getting chewed up too quickly, or they have lost so much blood so quickly because their doctors are just trying to get the iron down that they become low in hemoglobin or red blood cells. Rather than waiting for months for that to recover, you could be doing the supplements to lower the iron.”
Sutton’s husband also developed a pituitary tumor that was causing him to have high cortisol (Cushing’s disease). “Ultimately, I think the high iron created a lot of oxidative stress on his pituitary gland,” Sutton says. The only reason he was diagnosed early enough to save him was that they’d been checking his cortisol and DHEA on a regular basis.
“Periodically, they would jump up and then go back down. Then when the hemochromatosis got properly treated and the DHEA was still high, we were like, ‘Why is this happening?’ So we went to the endocrinologist and I said, ‘I’m worried my husband has Cushing’s.’ She was like, ‘He doesn’t have Cushing’s. He doesn’t look like somebody with Cushing’s. His hemoglobin A1C is normal.’
Five months later, he’s having surgery to remove the pituitary tumor. The reason I say that is because for years, he was told, ‘You just need to exercise and lose weight.’ His problem was not exercise. He had a pituitary tumor and hemochromatosis. Hemochromatosis was destroying his liver and his brain and his heart and everything else, and the pituitary tumor was causing him to have high cortisol, which made him look overweight.”
I believe progesterone may be one of the best ways to treat Cushing’s disease, as it very effectively blocks cortisol. Other natural substances that will inhibit cortisol include aspirin, DHEA, pregnenolone, emodin, vitamins A and D, gelatin or glycine, and niacinamide.1
The normal dose for progesterone is 25 to 50 milligrams. For Cushing’s, I would recommend about 300 mg. It’s virtually impossible to overdose on progesterone and there are no downsides to it. One caveat is that you need to administer it correctly to gain the optimal effects.
Avoid creams, pills and suppositories. Instead, mix pharmaceutical grade progesterone with the contents of one natural vitamin E capsule. Mix it with a paperclip or tiny spoon until all the powder is dissolved, then rub it on your gums. Vitamin E is the only natural compound that dissolves progesterone completely. For guidance on how to pick a good vitamin E supplement, see “The Four Hormones Most Adults Need More Of.”
As explained by Sutton, iron deficient anemia is a serious issue. Children born of women with iron-deficient anemia have significantly higher risk of low IQ, ADD, ADHD and other neurological issues that often do not go away with age.
“Many kids suffer from low iron, because they eat a lot of calcium rich foods. Calcium binds to iron, and then you get low in the iron. Maybe they’re picky eaters, they’re growing rapidly. So many kids are not being checked for their iron levels and they’re being diagnosed with ADHD when their problem is actually just low iron, because if you don’t have enough iron, you can’t make dopamine. So, low iron is a serious issue.”
People with iron-deficient anemia will typically have high TIBC and UIBC, as their bodies are trying to mobilize more iron. Serum iron and iron saturation will be low and ferritin will typically be below 30.
“Now, iron deficient anemia is more complicated in many ways because the question is, why are you low in iron?” Sutton says. “There’s so many reasons that you can be low in iron. Are you just not eating enough? Are you not absorbing it? I think the most common reasons that people develop low iron is because they have a GI bleed. They have intestinal malabsorption issues, maybe undiagnosed celiac disease.
There is a gene that can cause you to be more likely to have low iron. I have that gene and that gene actually causes you to make more hepcidin. With iron-deficient anemia you’ll also see low red blood cells sometimes, low hemoglobin and low hematocrit. MCH [mean corpuscular hemoglobin] might get low, MCV [mean corpuscular volume] might get low.”
One common cause for iron-deficient anemia is a deficiency in copper. Paradoxically, lack of copper is also a common cause for iron overload. Sutton explains:
“The reason for that is because copper is necessary for two key enzymes. The first one is called hephaestin and the second one is called ceruloplasmin. Hephaestin is in the lining of the gut, the intestinal lining. Copper is necessary for iron to be absorbed in the gut lining. So, without copper, you will not absorb iron and you will develop iron deficient anemia.
Once iron has been absorbed in the gut lining by hephaestin, it passes it off to ceruloplasmin, which is the second copper-rich enzyme. Ceruloplasmin basically then allows that copper to transfer in and then move throughout the body. So, without ceruloplasmin, iron gets stuck in the tissues. It’ll get stuck in the digestive system, it’ll get stuck in the retina, it’ll get stuck in the brain, it’ll get stuck in the liver.
So, you develop iron overload in the tissues. But eventually, if you’re low in copper long enough, you might then become low in iron, and then you don’t end up with all this extra iron in the tissues. The solution is take copper to fix that problem. That’s the way you solve copper-deficient anemia.
Copper-deficient anemia looks very similar to iron-deficient anemia if you’re looking at the iron panel. You’ll have a high TIBC, high UIBC, low serum iron, low iron saturation, low ferritin. You’ll also potentially see low neutrophils and low white blood cells, because you need copper to have normal immune function as well. So, you might be more at risk for infections.
Then of course you can look at the ceruloplasmin. I don’t find ceruloplasmin to be the easiest lab to look at, because it’s an inflammatory marker … If you’re taking hormones like estrogen or birth control or you’re pregnant or you’re just inflamed or have an infection, ceruloplasmin can jump around and go high.
If you have a low or low-normal ceruloplasmin, and then you take copper and ceruloplasmin goes up, that’s a good sign that you didn’t have enough copper.”
The best way to get iron is through your diet. Shellfish and beef are iron-rich foods with highly absorbable iron. That’s key, because there are two types of iron: heme iron and non-heme iron, the latter of which is not very absorbable. Heme iron is found in animal products while non-heme iron is found in vegetables such as spinach.
“If you’re not eating iron-rich foods like red meat, then you’re more likely to get low in iron if that is something that you struggle with,” Sutton says. “If you struggle with being high in iron, maybe you don’t want to eat as many of those things or maybe you just want to remove blood and supplement accordingly, so that you continue to eat those things.
The form that I like if I’m going to go to a supplement is ferrous peptonate, which I found to be the gentlest on my gut but also get the iron levels up. I really don’t like ferrous sulfate, which is the most common given iron. I don’t think it works very well, and it tends to create a lot of stomach pain. I always have to take my iron with food and sometimes I’ll add copper or vitamin C to it. If I don’t take it with food, it’s really going to upset my stomach.”
To learn more, check out Sutton’s books, “Genetic Testing: Defining Your Path to a Personalized Health Plan: An Integrative Approach to Optimize Health,” and “The Iron Curse, Is Your Doctor Letting High Iron Destroy Your Health?”
Many appreciate my openness to integrating new information into my personal health approach and what I teach. I am a perpetual learner and seek to constantly evolve my approach, so it is aligned with biological truth, even if I have to admit I was mistaken.
Along those lines, I only learned most of the information in this article earlier this year, and it has had a dramatic impact on how I view burning food for energy. This approach is dramatically different than I previously understood and recommended, which was focused on high-fat and low-carb consumption.
You might recall for the last few years I have warned that chronic low-carb eating is not a good idea, and that you need to cycle in and out of low carb. This was a great move in the right direction, but what I have recently learned is that it was not enough and that most people would benefit from far higher amounts of carbs.
When I first started keto, I was below 50 grams of carbs a day for about a year and then for the next five years increased to about 100 grams per day. For the past few months, I have increased that to 425 grams of carbs per day, mostly in the form of ripe fruit.
I have noticed dramatic beneficial changes in my blood work that I won’t go into now but will dive deep into in future articles. I will reveal that increasing my carbs by 400% resulted in a highly counterintuitive, 10% decrease in my fasting blood sugar, and that I also lost 10 pounds despite increasing the number of calories I was consuming — precisely the opposite of what most “experts” would predict.
This doesn’t mean you should stop what you are currently doing and switch, but if you have been struggling with keto and are unable to lose weight, it is likely that a high-fat diet is slowing down your metabolic rate, increasing your cortisol levels and contributing to an inability to achieve your ideal body weight.
My strong recommendation would be to not dismiss this concept as well-intentioned but seriously misguided nonsense, but to take the time needed to understand the solid science behind it.
The reason I switched to the higher carb, low-fat diet was due to learning the late Ray Peat’s work through his student Georgi Dinkov. Peat was a biologist and thyroid expert; Dinkov is a biohack expert. Since the beginning of the year I have been watching Georgi’s videos on YouTube for about two to three hours a day.
He has a thick Bulgarian accent and talks fast so you need to listen at 1X, although I typically watch his videos at least two to five times as it seems every time I relisten to them I learn something new or understand what he has to say in a new way.
Here is a chronologically sorted link to most of his past interviews.1 And wouldn’t you know it, he has not been censored by the globalists, so hundreds of hours are available for free on YouTube and it won’t cost you anything but your time to review.
However, please know that everyone is different and has a unique biochemistry, so your dietary program would have to be customized and fine-tuned for you. Many of the principles are universal and can be widely adopted, though, so If properly done I am convinced that most will notice profound improvement in their metabolic rate, mitochondrial function and energy levels, along with a reduction in inflammation.
One of the foundational concepts of health that I’ve had to radically revise my thinking on, based on Peat’s and Dinkov’s work, is the idea that eating a low-carb diet long-term is the best way to optimize your metabolic and mitochondrial health.
I now realize that this was misguided, and the reason for that has to do with the fact that your body requires glucose, and if you aren’t eating it you will go into a hypoglycemic coma and die. Obviously, your body has safeguards to prevent that, and the major one is the hormone cortisol.
In medical school, we learned that cortisol is a glucocorticoid. Gluco means glucose (sugar) and cortico means it comes from the adrenal cortex. It’s also another word for steroid. We were told that cortisol is responsible for maintaining glucose homeostasis, but led to believe its primary purpose was for inflammation.
Well, that is just not true. While cortisol certainly contributes to glucose balance, its primary purpose is to raise your blood sugar when it is too low and you don’t have enough glycogen reserves in your liver.
But just how does cortisol increase your blood sugar? It does it by breaking down your muscles, bones and brain. It sacrifices your lean muscle mass to release amino acids that your liver converts to glucose in a process called gluconeogenesis.
So, ultimately, cortisol also is going to increase inflammation and impair your immune function. And it increases food cravings. So, you do not want your cortisol to be elevated. For a long time, I was a proponent of a low-carb diet, but now I realize that chronic low-carb is not a good idea.
As a fuel, glucose is vastly superior to fat, and this was something I simply got wrong. The same thing goes for fasting. Both low-carb and fasting are great interventions in the short-term for those who are overweight and metabolically inflexible.
However, once you’ve regained your metabolic flexibility, it is important to revise your strategy and add healthy carbs back in, or these strategies will backfire and lead to decreased metabolic health, compromised mitochondrial function and impaired metabolism.
Cortisol happens to be the primary aging hormone. If it is chronically elevated, you simply will die prematurely as it is highly catabolic, meaning it will break down your body tissues. To stay healthy as you age you need to be anabolic and build healthy tissues like muscle and mitochondria.
Elevated cortisol will seriously impair those efforts. So, it is clear that you need to be doing everything you can to keep your cortisol levels and chronic inflammation low.
The Paradox of Simple Versus Complex Carbs
Since I recorded the video above, it has become clear to me why there is a problem with the seemingly paradoxical conclusion that simple carbs are better than complex carbs for most people. I did not understand this when I recorded the video.
I have since determined that this is a result of most people eating large amounts of metabolic poisons like linoleic acid (LA) their entire life, in addition to regular estrogen exposure in the form of plastics which are xenoestrogens. As a result of these exposures, they have dramatically altered the composition of their microbiomes.
This occurs because these metabolic poisons result in a decrease in cellular energy production in the mitochondria, which then decreases carbon dioxide production in the intestine. The relatively lower concentration of carbon dioxide in the large intestine promotes the growth of pathogenic disease-causing bacteria known as facultative anaerobes.
These specific bacteria have high amounts of lipopolysaccharide (LPS) embedded in their cell membranes. When they are provided with food in the form of complex carbohydrates, they serve as fertilizer to accelerate their growth, so they multiply and eventually die.
When they die, this LPS, otherwise known as endotoxin, is released, and that is another potent metabolic poison that will radically decrease your mitochondria’s ability to create cellular energy, thus contributing to a vicious downhill cycle.
This sets up the seemingly paradoxical scenario where healthy food such as complex carbohydrates can make your health worse, because they are increasing the concentration of endotoxin in your body, which in high concentrations can result in septic shock that kills you.
The solution is to improve your health by improving your mitochondrial function and their ability to create sufficient cellular energy, which will subsequently restore the balance of healthy bacteria in your gut. When this is achieved, then complex carbohydrates transition to becoming very healthy.
But until your mitochondria produce adequate energy, complex carbs frequently contribute to worsening your health through the production of endotoxin. So it’s wise to carefully navigate with the introduction of complex carbs if you have been exposed to metabolic poisons for most of your life.
I believe the most prudent strategy is to listen and trust your body. If you have any problems eating complex carbs that result in bowel symptoms, then it would be wise to consider restricting your carbs to very simple carbohydrates such as fruit juice, which is the easiest carbohydrate to digest.
Once that is tolerated then you can go to healthy whole fruits. Once that is tolerated then you can progress to including other more forms of more complex carbohydrates until you are feeling that you can tolerate those.
It would be a major mistake to increase your carb intake if you are still on a high-fat diet. I did this experiment in the mid-‘80s after I read the book by Harvey and Marilyn Diamond called “Fit for Life.”
They suggested having fruit only for breakfast – which I tried. Then I did my lab work and found my fasting triglycerides and lipoprotein profiles had exploded for the worse. I prematurely concluded that a high fruit diet was nonsense and remained relatively low-carb for nearly four decades.
This was until I encountered Ray Peat’s work and reevaluated my initial impression. I now understand that I was missing important parts of the strategy. And now I eat 3 to 4 pounds of watermelon every morning at 5:30 as my first meal, followed by three eggs and 8 ounces of white rice and 2 ounces of maple syrup one to two hours later.
That sounds like a lot of carbs, and it is. I have additional fruits later in the day and now my carb intake is about 425 grams a day. You might wonder what has happened to my weight and blood sugar with all these extra carbs.
Well, I thought my weight was good at 192 as I increased my muscle mass, but it has decreased by 10 pounds to 182 with no change in muscle mass. My fasting blood sugar has dropped 10 points and, so far, it seems to be working for me.
This is one of the most important principles in food science that I had never learned or understood until recently. My strong guess is that this is also true for most natural medicine clinicians. That is why I created the figure below to help you visualize it, so you can better understand this vital concept.
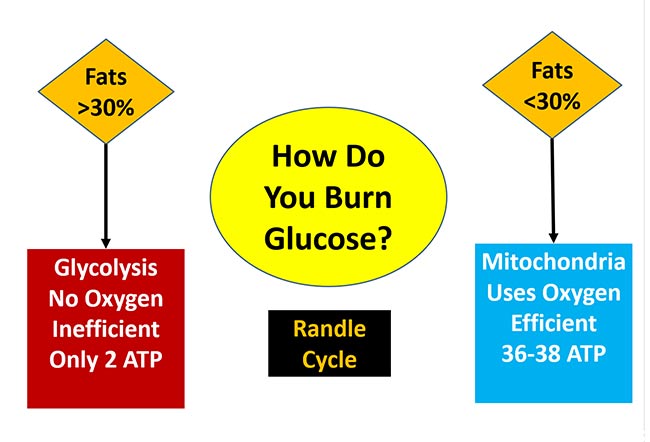
Low-carb diets have helped at least tens of millions of people improve their health for a very good reason, and that is there is a stealth switch that controls what fuel your mitochondria can burn. They can only burn one fuel at a time, either fat or glucose.
The switch has been given the name the Randle cycle, but it is more helpful to visualize it as a railroad switch that changes the tracks of the train. The train can only travel down one track; not both. This is because only one type of fuel can be burned at a time.
The best-case scenario is you metabolize, or burn, glucose in your mitochondria without any reductive stress (a term I will explain in my upcoming interview with Georgi Dinkov). When you do this, you will only generate 0.1% reactive oxygen species (ROS).
Not only does this route generate less ROS, but it also is incredibly efficient at energy production by creating 36 to 38 Adenosine triphosphates (ATP) for every molecule of glucose that is metabolized. It will also generate metabolic water and carbon dioxide, which are also important for your health.
For this to occur, as indicated in the figure above, you will need to consume less than 30% of your calories as fat. When you consume significantly more than that amount, the switch changes to burn fat in your mitochondria and you will not be able to burn glucose until your fat decreases to less than 30% of calories.
Since glucose is unable to be shuttled into the mitochondria to burn, it winds up backing up into your bloodstream, raising your blood sugar. This is a major contributor to diabetes. What little glucose is burned for fuel is done by using glycolysis, which is a primitive pathway that bacteria and cancer cells use.
It is great that we have this pathway, as you absolutely need it for quick fuel when you are activating your type II muscle fibers. But if this is the primary way you burn glucose, you are in a catastrophic metabolic state as you are creating loads of lactic acid as a waste product instead of healthy CO2. And, you are only generating two ATP for every molecule of glucose, which is 95% less energy.
Lactic acid increases reductive stress, which causes reverse electron flow in the mitochondria and causes reductive stress, which increases the ROS to 3% to 4%, which is 30 to 40 times more than when glucose is burned efficiently in the mitochondria. You likely don’t yet understand reductive stress, the opposite of oxidative stress, but I will be doing an interview with Georgi on this and will be posting it later this month.
Remember, when you are burning glucose efficiently in your mitochondria, the glucose is converted not only to 36 to 28 ATP, but when the electrons from the glucose are ultimately handed off to oxygen, metabolic water (deuterium free) is made and, very importantly, carbon dioxide.
This is vital to understand as carbon dioxide is a potent stimulator of mitochondrial biogenesis which will increase the number of mitochondria that you have so you can make even more energy.
Conversely, when you are burning glucose far less efficiently in glycolysis you are only generating two ATPs, and rather than creating life-sustaining carbon dioxide, you are generating life-damaging lactic acid, which will degrade your mitochondria and make them die sooner.
In this second video, anti-vegan activist Paul Saladino interviews Dinkov about the Randle cycle. Dinkov comments:
“The first accusation against you, that whole milk will somehow make you fat because of the Randle cycle [is] misguided because if you look at the label, whole fat milk has like 5 grams of fat per serving but 12 grams of carbs, so you’re actually [getting] more carbs.
But let’s talk about meat. Most meats … are actually not that high in fat, and a lot of the fat in them is actually short chain fatty acids, which are not subject to the Randle cycle because they get transported into the cells through a known L-carnate-independent mechanism.
They metabolize similarly to sugar, and they don’t seem to be triggering the same sort of Randle cycle effect. Now, what drives the Randle cycle effect? When you’re oxidizing primarily fats … the master conductor redox modulator — which is the NAD to the NADH ratio, specifically the intra-mitochondrial one — drops. (This simply means the more NAD+ the better).
Basically, the NAD to the NADH ratio — which signals how oxidized versus how reduced you are, metabolically — [is] the primary regulator of whether the pyruvate dehydrogenase (PDH) will accept pyruvate and convert it into acetyl-CoA and then continue with the Krebs cycle in the electron transport chain, or not.
(Pyruvate is the three-carbon molecule breakdown product of glucose. PDH is the enzyme that converts it to acetyl-CoA which allows it to enter the mitochondria and be burned efficiently. If PDH is inhibited, it will force your body to use fat).
In other words, a high ratio of NAD to NADH (meaning high NAD+) when you’re very oxidized favors the activity of pyruvate dehydrogenase, so you will not be accumulating pyruvate [and] you will not be generating lactate.
But if you’re eating a lot of fat, the NAD to the NADH ratio drops, and then the buildup starts to happen. Pyruvate accumulates, lactic [acid] accumulates. [This means] the Krebs cycle is working because it’s accepting acetyl-CoA from the beta oxidation. That’s how the fatty acids get oxidized.
So, that’s the gist of the Randle cycle … If you’re providing a lot of glucose, in theory you should be able to out-compete the free fatty acids and oxidize more glucose versus fat, but that all depends on how much glucose can get into the cell.
And, unfortunately, when you’re eating these high-fat diets, when you have higher lipolysis, the actual uptake of glucose into the cell is already largely blocked …
Free fatty acids not only block the metabolism of glucose, they also block the uptake of glucose into the cell. So, they prevent the positive effects that the glucose would have had, in terms of competing with the free fatty acids …
Basically, too much fat blocks your uptake and utilization of glucose, and whatever glucose is taken up, you largely convert to nonbeneficial byproducts such as lactic acid …”
So, to summarize Dinkov’s rather complex exposition on the Randle cycle’s effects: a) fats can make you fat directly; and b) fats limit your ability to metabolize glucose. This is due to the Randle cycle’s preference to fat metabolism when more than 35% of your calories come from fats. And, even if you metabolize small amounts of glucose, your body will favor the conversion of glucose into fat versus ATP, water and carbon dioxide.
This is because the enzyme PDH, which converts the glucose metabolite pyruvate, is inhibited by high fat concentrations, and won’t convert pyruvate to acetyl-CoA to be burned in the mitochondria. Instead, because PDH is inhibited, the pyruvate is metabolized into lactate. This entire process is antimetabolic and slows down your metabolism, increases your ability to gain weight, and lowers your ability to generate cellular energy.
So, when more than 30% to 35% of your calories are coming from fat, you are forcing your cells to burn fat and put glucose on the back burner, instead of being metabolized like it should be.
Clearly, the most important strategy to help your metabolism is to avoid eating linoleic acid at all costs. It is impossible to avoid as it is in nearly every food, but you want to keep your levels below 2% of your daily calories. This means avoiding ALL processed foods and typically most restaurants.
A powerful strategy that nearly everyone should do is to make sure that you are taking a high-quality vitamin E supplement once a day. Why? Because most everyone has 20 to 30 times more LA in their body than optimal. Not only will vitamin E impair the release of it from fat cells, but once released it will help protect the LA from converting into dangerous oxidized linoleic acid metabolites (OXLAMs).
Most vitamin E supplements should be avoided, so how do you identify a high-quality vitamin E supplement? It should have most of the vitamin E isomer as alpha tocopherol, typically about 150 units. It should also have the other tocopherol isomers: alpha, beta and gamma, but at far lower doses.
Additionally, it should have alpha, beta and gamma tocotrienols. Finally, it should only have the “D” isomer. Avoid all vitamin E supplements that are “DL,” which are 50% of the wrong isomer.
It would be very wise to make sure you have enough NAD+ as it will also inhibit the release of LA from your fat cells. If you haven’t read and viewed by interview with molecular biologist Nichola Conlon on this topic, you can read it on my Substack. Sadly, NAD+ decreases dramatically as you age, which leads to nearly a 1-to-1 reduction in ATP, your cellular energy currency.
Fortunately, this can be inexpensively addressed by taking 50 mg of niacinamide three times a day. More is not better, so avoid 500 mg tablets as they will impair your longevity proteins. Typically, one sixty-fourth of a teaspoon of niacinamide powder is about 50 mg.
Finally, aspirin can be a very useful way to inhibit LA lipolysis. Aspirin is a very interesting approach and I go into far more details in my recent article on it.
I previously touched on the Randle cycle in “How the Wrong Dietary Fat Can Wreck Your Health,” which also featured an interview with Dinkov. In that interview, Dinkov cleared up several areas of confusion, including the following:
•Low-carb dieting is a great short-term intervention for people who are overweight and insulin resistant. Lowering carbs will help reset your metabolism and recover your metabolic flexibility. However, in the long-term you will likely run into trouble — especially if you’re also doing a lot of endurance training.
One of the reasons for this is because when you’re in a low-carb state, lipolysis is elevated, which releases inflammatory polyunsaturated fatty acids (PUFAs) such as LA from your cells that are then into dangerous OXLAMs (oxidative linoleic acid metabolites) that will damage your tissues.
PUFAs such as LA are not digested. Instead, they’re stored.2 Most of the body fat in obese individuals is composed of PUFAs, not saturated fat. Saturated dietary fat is mostly burned (oxidized) and used up. So, most people have large stores of LA, and these stores need to be lowered to safe levels of 1% to 2% LA.
•Extended fasting and using an excessively narrow time-restricted eating (TRE) window can also backfire once you’re metabolically flexible, as it too helps push LA out of your cells.3,4,5,6,7,8,9,10 An extreme example of TRE is the one meal a day (OMAD) protocol, where you’re fasting 22 hours or more each day. Dinkov believes this is too extreme for most people.
The half-life of PUFAs such as LA, which get embedded and integrated into your cell membranes, is about 680 days. This means that ridding your body of LA will take approximately seven years, provided you don’t load more in. And you really do want to get rid of this fat, as it’s highly inflammatory and prevents your mitochondria and cellular machinery from operating properly. But you need to do it slowly and methodically.
Exercise and fasting will help drive the LA out, but you need to be really careful if you have a lot of LA storage. You want to avoid excessive lipolysis — any situation where you’ve run out of glycogen, which can easily happen when you’re not eating for long periods, when you’re on a chronic low-carb diet, and/or when you’re engaging in intense exercise, especially if you exercise in a fasted state.
•Chronic long-term, low-carb, and chronic extended fasting also result in elevated cortisol, which is highly inflammatory and promotes the storage of fat. Elevated cortisol is also highly catabolic and will cause you to lose lean muscle mass so your liver can make glucose. For these reasons, low-carb diets and fasting are best implemented as temporary strategies to restore metabolic flexibility.
With all of that in mind, how can you safely reduce your LA stores without self-sabotaging? Extensive fasting will, in this instance, backfire, as will overtaxing yourself with heavy exercise. You’ll need to accept that achieving optimal health is a marathon, not a sprint, and that it’s going to take years to purge your LA stores. Dinkov suggests the following strategy:
So, to recap, temporarily implementing a six- to eight-hour time restricted eating window, or even longer eating restrictions and fasts, is appropriate for anyone who is insulin resistant and metabolically inflexible — and that’s about 95% of the population.
However, once you lose your insulin resistance and become metabolically flexible — which typically takes a few weeks — you’ll want to increase your eating window to eight to 12 hours to avoid elevating your cortisol, as cortisol promotes chronic inflammation that can lead to tissue damage, and promotes the storage of fat.
How does TRE and extended fasting raise cortisol, you ask? It is important to understand that cortisol is a powerful hormone whose primary purpose is to shred your lean muscle mass and bones to obtain amino acids for your liver so it can produce glucose. This is cortisol’s primary role. If your blood sugar gets too low, you will go into a hypoglycemic coma and die. Your brain requires sugar and if it doesn’t get it, it is game over.
Usually, it takes a few weeks and occasionally longer, for you to recover your metabolic flexibility. During those first three to six months, stick to a six- to eight-hour eating window. Once you’re metabolically healthy, avoid eating windows under eight hours. I’ve now shifted to a schedule where I always have an eating window of more than eight hours a day and closer to 12, in the summer when there is plenty of daylight.
Interestingly a recent study showed that a lower fat, higher carb approach lowers the risk of death by 30%, while with the converse a high-fat, low-carb diet increases the risk of death by 30%.11,12 So, it’s your choice for sure, but I am convinced that having more healthy carbs than fat is a great choice to improve your metabolic health.

Written By: GreenMedInfo Research Group
Arthritis, affecting millions globally, presents a significant health challenge. This condition, characterized by joint pain and inflammation, varies in severity and type, including osteoarthritis and rheumatoid arthritis. Conventional treatments typically involve non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids, and disease-modifying antirheumatic drugs (DMARDs), which, while sometimes effective at reducing symptoms, can pose serious health risks such as gastrointestinal bleeding, liver and kidney damage, and increased risk of heart problems. Emerging research highlights various natural alternatives that might offer comparable or superior benefits without these risks.
The following 10 substances have been researched for their potential value in addressing arthritis naturally:
Conclusion
These findings underscore the potential of natural approaches in managing arthritis, providing alternatives to conventional drug therapies.
© March 4th 2024 GreenMedInfo LLC. This work is reproduced and distributed with the permission of GreenMedInfo LLC. Want to learn more from GreenMedInfo? Sign up for the newsletter here www.greenmedinfo.com/greenmed/newsletter.
For full references please use source link below.
Carnitine is another important nutrient that’s abundant in animal foods. Your body produces L-carnitine from the amino acid lysine, and while healthy people are typically able to synthesize enough, certain conditions — like pregnancy — may cause your body’s need for carnitine to exceed its ability to produce it. For this reason, carnitine is considered a conditionally essential nutrient.1
L-carnitine and acetyl-L-carnitine are forms of carnitine found in dietary supplements. While your body absorbs carnitine from animal foods such as grass fed beef better than carnitine in dietary supplements,2 some research suggests L-carnitine supplements may benefit certain conditions.
Your body needs carnitine for energy production. It helps transport long-chain fatty acids into your mitochondria where they’re oxidized and turned into energy in the form of adenosine triphosphate (ATP),3 which is needed by your cells for life, repair and regeneration. Carnitine may also help remove toxins from the mitochondria.4
Acetyl-L-carnitine (ALCAR) is more easily absorbed in your gut than L-carnitine, and also crosses the blood-brain barrier.5 ALCAR has many beneficial effects on brain metabolism, protects against neurotoxic insults and has been shown to benefit certain forms of depression. In one study,6 healthy mice given ALCAR for 25 days at a dose of about half a gram per kilo were found to have increased levels of the neurotransmitters noradrenaline and serotonin.
According to the authors, this is “consistent with ALCAR’s potential efficacy for depressive symptoms.” In another study, ALCAR was found to improve the clinical condition of patients with degenerative cerebellar ataxia, a condition resulting in the loss of control of bodily movements.7 According to the authors, “statistically significant improvement of some symptoms and a slow progression of the disease in both groups of patients” were observed.
Carnitine is also being studied for use in Alzheimer’s disease. According to the National Institutes of Health:8
“Cholinergic neurons use the neurotransmitter acetylcholine, and Alzheimer’s disease is often treated by increasing acetylcholine levels or preventing its breakdown. Carnitine might be conditionally essential in individuals with Alzheimer’s disease because it may support acetylcholine synthesis and help remove toxic compounds to alleviate mitochondrial dysfunction associated with extensive degeneration of brain structures.
Therefore, researchers have examined whether acetyl-L-carnitine supplements benefit individuals with Alzheimer’s disease or other forms of dementia, but studies have had mixed results.”
In a meta-analysis of 21 studies, adults with mild cognitive impairment or Alzheimer’s disease took 1.5 grams to 3 grams of acetyl-L-carnitine or placebo daily for three to 12 months. Those taking acetyl-L-carnitine had greater improvements than those taking placebo.9,10
It’s also been widely studied for autism as a treatment that targets mitochondria. One meta-analysis found low carnitine in 80% of children with autism.11 As explained in Seminars in Pediatric Neurology:12
“Two medium sized (n = 30, 30) double-blind placebo-controlled studies using L-carnitine treatment (50 mg/kg/d for 3 months and 100 mg/kg/d for 6 months) found that scores on the Childhood Autism Rating Scale (CARS) improved with L-carnitine as compared to placebo with one study finding that greater symptomatic improvement was correlated with a greater increase in blood carnitine levels.
A small (n = 10) 8-week open-label trial of L-carnitine used particularly high doses (up to 400 mg/kg/d in 3 divided doses, maximum of 6000 mg/d) …
Several parental rated measures showed improvements in behavior and hyperactivity before correction for multiple comparisons and improvements in language correlated with post-treatment blood carnitine levels. Children with ASD and genetic mutations in the carnitine pathway also appear to response to L-carnitine.
… Thus, L-Carnitine is a promising treatment for children with ASD. For child neurologists, it is always important to remember that children with ASD could have an underlying defect in carnitine metabolism.”
Carnitine for Heart Health
There’s some evidence that carnitine may help moderate oxidative stress and decrease inflammation, benefitting heart health. It may also help prevent potentially fatal arrhythmias, or irregular heart rhythms.13
One meta-analysis involving 3,629 adults found, “Compared with placebo or control, L-carnitine is associated with a 27% reduction in all-cause mortality, a 65% reduction in Vas [ventricular arrhythmias], and a 40% reduction in anginal symptoms in patients experiencing an acute myocardial infarction.”14
There’s some controversy over carnitine for cardiovascular disease, however, because it’s metabolized by gut microbiota into trimethylamine-N-oxide (TMAO), a substance associated with an increased risk of cardiovascular disease,15 although the evidence on that is mixed.
According to James DiNicolantonio, Pharm.D., who is also the coauthor of my book, “Superfuel: Ketogenic Keys to Unlock the Secrets of Good Fats, Bad Fats, and Great Health,” the likely true cause of elevated TMAO levels is hepatic insulin resistance.16 Because carnitine (and choline) raises TMAO, some recommend limiting dietary and supplementary intake of these nutrients.
However, DiNicolantonio and his coauthors point out there’s a significant flaw in this theory, stating, “… supplemental carnitine is known to be highly protective in patients with vascular disease; and fish, the richest dietary source of preformed TMAO, is also protective.”17 There’s little evidence to suggest that dietary intake of TMAO or its precursors actually promote CVD, provided your renal function is normal. DiNicolantonio explains:18
“With respect to carnitine and CV risk, a meta-analysis19 of prospective clinical trials in patients who had recently experienced a myocardial infarction concluded that carnitine supplementation is markedly protective with respect to total mortality, ventricular arrhythmias and new-onset angina …
Clinical trials20,21 have also reported favorable effects of supplemental carnitine or carnitine esters on angina, intermittent claudication and heart failure.
Moreover, rodent atherogenesis studies, in which carnitine has been administered in doses reasonably proportional to the supplementation doses used clinically, have found that carnitine is anti-atherogenic, despite its propensity to raise TMAO …
It is therefore reasonable to suspect that moderately elevated TMAO, rather than being a mediator of the associated CV risk, is a marker for factors which both promote CV events and increase plasma TMAO.”
Research suggests L-carnitine supplements, which are the least expensive form on the market with an absorption rate of 14% to 18%,22 may be useful for weight loss. In a systematic review and meta-analysis of 37 trials, L-carnitine supplementation significantly decreased body weight, body mass index and fat mass, particularly in adults who are overweight or obese.23
“A nonlinear dose-response association was seen between L-carnitine supplementation and body weight reduction … suggesting that ingestion of 2000 mg L-carnitine per day provides the maximum effect in adults,” the team, from Shahid Sadoughi University of Medical Sciences in Iran, noted.24
L-carnitine concentrates in the epididymis, a duct behind the testis where sperm mature. Concentrations of L-carnitine in semen have been linked to the number of sperm, suggesting it may play an important role in fertility in men. Some research also shows that L-carnitine supplementation for two months may improve sperm quality and motility.25 According to the NIH:26
“Carnitine might play a role in sperm maturation, sperm motility, and spermatogenesis. It might also reduce oxidative stress, which could improve oocyte growth and maturation. Therefore, researchers are examining whether supplemental carnitine improves sperm count, concentration, and motility as well as pregnancy rates.”
Women with polycystic ovary syndrome (PCOS), which can affect fertility, may also benefit from carnitine. A systematic review and meta-analysis involving women with PCOS revealed that carnitine supplementation ranging from 250 mg to 3,000 mg daily for 84 to 90 days significantly improved ovulation and pregnancy rates, while reducing BMI and insulin resistance.27
There’s interest in the use of carnitine to enhance athletic performance, in part because carnitine preserves muscle glycogen while boosting fat oxidation. “It also spares the use of amino acids as energy sources during exercise, making them potentially available for new protein synthesis, and decreases the accumulation of lactate,” NIH notes,28 but research is mixed on its benefits.
In one study published in the Journal of Physiology, the data showed L-carnitine supplementation for six months raised levels of muscle carnitine by 21%.29 Further, participants taking carnitine supplements raised their athletic performance and work output by 11% in a 30-minute performance trial.
The researchers explained this improvement “by the dual role of carnitine — glycogen sparing at low intensities and reduced muscle lactate accumulation at high intensities.”30
Where carnitine further shines is for those with frailty. It’s been suggested that carnitine deficiency could cause frailty via mitochondrial dysfunction, with research showing pre-frail older adults had decreases in frailty and improvement in hand grip strength when they took 1.5 grams of carnitine daily for 10 weeks.31
Additional research is looking into the effects of carnitine supplementation on nonalcoholic fatty liver disease (NAFLD). A systematic review and meta-analysis revealed that L-carnitine supplementation may improve liver function and regulate triglyceride metabolism in those with NAFLD. Writing in Systematic Reviews, researchers explained:32
“The main drivers in NAFLD are inflammation and accumulation of lipids, and L-carnitine has been shown to have anti-inflammatory effects by upregulating the peroxisome proliferator activator receptor-γ (PPAR-γ) in the liver. L-carnitine is also closely related to fat metabolism.”
Beyond the liver, carnitine also shows promise for a range of other health conditions, including:33,34
In another example, a systematic review and meta-analysis found men and women experienced improvements in waist circumference and blood pressure, two biomarkers of metabolic syndrome, when taking carnitine supplements.35
The studies used carnitine doses between 0.75 grams (gm) and 3 gm per day for eight to 24 weeks, with researchers suggesting biomarkers of metabolic syndrome could improve with a carnitine dose of 1 gm to 3 gm per day, by reducing fasting blood sugar and triglycerides, while increasing high-density lipoprotein (HDL) cholesterol.
Most people can effectively synthesize between 11 mg and 34 mg of carnitine per day, which is typically enough to prevent deficiency.36 Animal foods, including meat, seafood and dairy, are the richest sources of L-carnitine, so if you eat animal protein it will virtually assure you receive enough carnitine without having to take supplements.
However, if you eat a primarily plant-based diet or are targeting certain conditions, you may need to consider supplementation. Acetyl-L-carnitine (not regular L-carnitine), for instance, appears to be particularly beneficial for improving memory, but you need about 2,000 mg to 2,500 mg a day. Most notice a difference after a few weeks.
If you do choose to supplement, be sure to choose a reputable source. When NOW Foods tested seven largely unknown brands of acetyl-L-carnitine, none met label claims and most were labeled incorrectly.37