Craig Kelly writes:
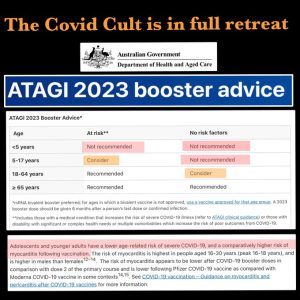
Australian Technical Advisory Group on Immunization made U-Turn and removes booster recommendation on anyone under 65 citing risk of vaccination induced myocarditis!
ATAGI now recommends AGAINST all children 5 & under from being jabbed.
They also now recommend AGAINST healthy teenagers & kids 5-17 from being jabbed.
Even for healthy adults the guidelines are now only “consider”.
The chief warlocks of insane Covid Cult are now in full retreat – swamped by a tsunami of evidence showing the risks (including death) of these experimental genetic shots are greater than any potential short term benefit.
But this was clear from the start. ATAGI were nothing but malfeasant puppets of Big Pharma
So now will the malfeasants at APHRA reinstate the doctors who they cancelled for saying exactly what ATAGI are saying now?
Will human rights abusing CEO’s like Qantas’s Alan Joyce now drop all coercive mandates?
Will the sociopath Dan ‘vaccines work’ Andrews public state that his beloved jabs are no longer recommended because they are not sufficiently safe nor sufficiently effective?
And will the ABC report any of this?