This is gold. Take your time to study…
https://www.andrewbridgen.com/news/list-supporting-references-used-vaccine-harms-debate-speech

Tom's Blog on Life and Livingness
This is gold. Take your time to study…
https://www.andrewbridgen.com/news/list-supporting-references-used-vaccine-harms-debate-speech
A Research Gate study uncovered a mysterious toxin behind autoimmune disease:
A 50-year-old woman had been suffering from pain and fatigue for more than 10 years.
Her debilitating symptoms lead to a fibromyalgia diagnosis.
Strangely enough, during a vacation in a foreign country, her pain and exhaustion suddenly vanished…
However, her symptoms reappeared in the days following her return home…
Which made her believe something she was eating or drinking might have caused her the symptoms.
And she was absolutely right.
As it turns out, when she was home, she used aspartame as a sugar replacement.
After she excluded aspartame from her diet, her autoimmune disease vanished completely.
Aspartame is just one of the many toxins associated with autoimmune disease.
My research team and I have found 23 toxins in our food that are even more dangerous…
Download my eBook, 23 Toxic Threats in Our Food that Trigger Autoimmune Disease & How to Reverse Their Effects now and see if these toxins could be the trigger for your autoimmune symptoms:
In this eBook, you will also find time-tested tools to reverse autoimmune symptoms, even if you think your case is too severe…
But you must hurry, this eBook is only available for a very limited time.
When you download this eBook you’ll also get free access to my 10-episode docuseries, Autoimmune Answers that reveals the most effective natural protocols for actually reversing autoimmune disease!
Click here to download your copy at no cost: https://theautoimmuneanswers.com/23-toxic-threats/
To your health,
Jonathan Otto

What is the World Health Organization, and what is it for, really? In the Children’s Health Defense (CHD) video above, Dr. Meryl Nass interviews investigative journalist James Corbett of The Corbett Report about the weaponization of the WHO. Nass also published a Substack with additional background information for this episode.
The WHO is actually a specialized agency within the United Nations. It was initially established in 1948 to “further international cooperation for improved public health conditions,” but we can now see that the long-term goal of the WHO is to serve as a foundation or hub for a one world government under the auspice of coordinating and ensuring global biosecurity.
This becomes self-evident when you review the proposed amendments1 to the existing International Health Regulations (IHR) and the new pandemic treaty, which Nass and Corbett review in the featured video.
I also provided details about the treaty in “What You Need to Know About the WHO Pandemic Treaty.” Below, I will primarily focus on the proposed amendments to the International Health Regulations (IHR).
In a December 16, 2022, Substack article,2 James Roguski also reviewed how a temporary crisis (the COVID-19 pandemic) — which, by the way, is long since over — is being used by the WHO to seize permanent power.
Background to my interview with James Corbett, as requested by a reader: https://merylnass.substack.com/p/background-to-my-interview-with-james

Use it or lose it!
Motion is lotion.
Eat less and move more.
The journey to health and wellness might start with the first step but prior to that is the decision to improve!
Feng Fu Point
(Tom: Passing this on as received. I have no experience with it so would be interested in hearing from someone who has tried it.)
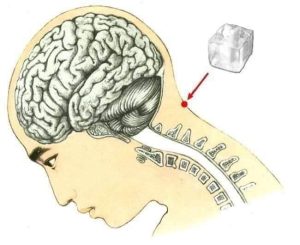
What happens when you place an ice cube beneath the base of your skull for twenty minutes?
Traditional Chinese medicine has discovered a point in our body that when stimulated promotes overall well-being. This point called Feng Fu is the pressure point located behind the head, at the base of the skull, on top of the neck.
FENG FU POINT:
According to Traditional Chinese Medicine, this method restores the body’s natural physiological balance – giving a strong injection of life, rejuvenating the whole body.
Technique of applying an ice cube on a Feng Fu point:
Choose a comfortable position lying on your stomach face down.
Apply an ice cube one to two times per day for 20 minutes.
If it better suits you, you can use a cloth or a plastic baggy to encase the cube of ice before applying on the feng fu point.
Note: After 30 seconds, you may begin to experience a slightly warm sensation.
In the first few days of utilizing this technique, you may experience feeling of slight euphoria due to the release of endorphins igniting within the Feng Fu Point.
These are some of the changes you may experience using the Feng Fu Point method:
– Reduction of headaches, teeth pain and joint pain.
– Blood pressure problems regulating.
– Regeneration in the digestive system.
– Restored sleep / mood.
– Relieving gastrointestinal infections.
– Relieving neurological and psycho-emotional disorders, chronic fatigue, stress, depression, and insomnia.
– Spinal degeneration change.
– Breathing problems improving.
– Helping inhibit cardiovascular problems.
– Elimination of common colds.
– Stabilization of thyroid disorders.
– Relieving asthma attacks.
– Cellulite reduction.
– Gastrointestinal disorder recovery.
– Obesity and malnutrition disorders improving.
– Disorders related to impotence and infertility alleviated.
– Menstrual disorder recovery.
– Kim Chi | Via Lionel Dupont


It’s starting, Bill Gates announces the next pandemic date and outbreak location…

Kary Mullis invented the PCR test so has played a key part in the recent drama.
https://flote.app/post/b3b52b0b-188c-45b9-bda0-35d6fb430477

