Ready for a laugh?
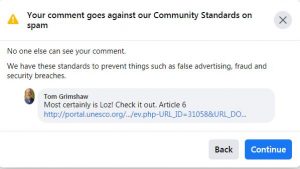
Twice, once yesterday and once the day before, I posted a link to the Universal Agreement on Medical Bioethics and Human Rights to illustrate to people that mask mandates (let alone quarantine, lockdowns, enforced vaccination etc.) are illegal and violate our country’s international agreements and our personal human rights.
This morning I logged on to find that my comments had been flagged as spam. They do not fit the agenda, obviously! LOL!
When you see how desperate they are to suppress the truth and maintain the facade it is truly laughable!