
How the UN is Holding Back the Sahara Desert
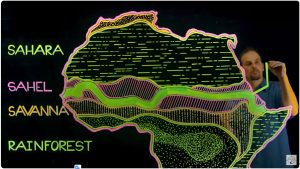
Permaculture instructor Andrew Millison journeys with the UN World Food Programme to the Northern border of Senegal to see an innovative land recovery project within the Great Green Wall of Africa that is harvesting rainwater, increasing food security, and rehabilitating the ecosystem.
Of Spike Proteins and Rabies: How the Spike Protein Mimics Rabies Axonal Degeneration and May Explain Many Sudden Deaths
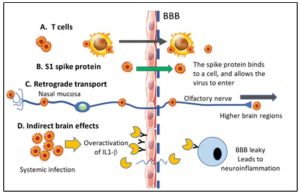
This article https://wmcresearch.substack.com/p/of-spike-proteins-and-rabies-how details another mechanism of harm from the spike protein which Walter calls “The Swiss Army Knife of Death”. If you have had Covid or the shot or feel worse after being exposed to others who have had Covid or the shot (shedding), please read and apply my compilation of how to detox yourself from those adverse effects: https://www.tomgrimshaw.com/tomsblog/?p=35644
I have subsequently created my own Anti-Spike Blend. Read the snippets of articles on the About tab of this page: https://www.healthelicious.com.au/NutriBlast-Anti-Spike.html
then get an Anti-Spike Blend from me or someone else. I believe mine is the most comprehensive but do your own due diligence.
Frank Zelenko Writes on X/Twitter:
I’m reasonably sure that Dr Zelenko worded everything below as it appears:
I’m tired of all the politically correct rhetoric. It is time to simply explain what happened and why.
1. Covid-19 is a man made weapon of mass murder that was funded and created by the American government and NIH
2. The American government serves the globalist elites and is the enemy of the people
3. Successful treatments were and are intentionally suppressed. Anything that gave people hope and reduced fear was obstructed
4. Global fear is used to fool people into taking mRNA shots
5. The mRNA shots were created to accomplish a globalist agenda
6. The globalist agenda is to
-decrease the world population and cause infertility
-to control and enslave people by injecting tracking technology and link that technology to the use of global cryptocurrency
-trans-humanist agenda through the mRNA delivered gene editing technology
Don’t fear covid. Don’t take mRNA shots
Form military tribunals and bring ALL the global predators to justice
All this can and will be proven with evidence
I’m a conspiracy realist
Vladimir Zev Zelenko
How Do Vaccines Cause Autism?
A Midwestern Doctor writes:
One of the most challenging things for me throughout my time in the medical field has been watching children become neurologically damaged by vaccines, and the widespread blindness of the medical profession to this issue. Unfortunately, because so much money has been spent to engineer the societal belief that vaccines do not cause autism, anyone that asserts otherwise is immediately subject to widespread ridicule, to the point it’s mostly a lost cause to convince medical professionals vaccines aren’t always safe. In many cases, the only thing that can open their eyes is their own child being severely injured.
The business of using propaganda (public relations or PR) has gradually evolved into a more and more streamlined formula that reuses the PR techniques found to be the most effective for manipulating the public. Because of this, once the COVID-19 vaccine push started, those who already had firsthand experience with the PR techniques used to prop up the previous vaccinations immediately recognized that something bad was in the works. More importantly, since the exact same vaccine PR scripts were reused to gaslight those with COVID-19 vaccine injuries, it led many to begin questioning the earlier scripts, like those used to debunk any link between vaccines and autism.
1. Contrary to popular belief, there is actually a great deal of compelling evidence linking vaccines to autism. For example, regressive autism always develops shortly after vaccination—but never before, something that cannot happen unless one causes the other. Likewise, there is a significant amount of evidence correlating vaccine uptake with autism rates.
2. There is presently no accepted explanation for what is causing the explosion of autism we are facing.
3. The explosion of autism is one of the costliest diseases facing our country, so decades of hand waiving that has insisted there’s no scientifically valid explanation for this explosion doesn’t cut it.
You might notice how these three points mirror what we are now seeing with the massive wave of (often unmistakable) side effects from the COVID-19 vaccines.
Keep reading: https://www.midwesterndoctor.com/p/how-do-vaccines-cause-autism
How Hanging for 2 Minutes Transforms Your Body (Science Explained)

Here’s a video on it:
https://www.youtube.com/watch?v=IymQ1VA3h2k
And Dr Mercola writes:
STORY AT-A-GLANCE
- When you dead hang you use gravity to free muscles around your shoulder — like the lats and chest — that can become stiff from sitting at a computer
- This movement can reshape the bone surrounding your shoulder to make more space in the ball and socket joint so your shoulder can move more freely
- The dead hang exercise also increases your grip strength, which is one of the biggest predictors of mortality
- A good target hang time is 90 seconds for men and 60 seconds for most women. Though longer durations are possible, it’s more beneficial to aim for shorter, more frequent sessions
- A digital hand dynamometer is the easiest and most reliable way of measuring your hand strength, and owning one can help you keep track of your grip strength over time
When you dead hang you use gravity to create space in your shoulders that are typically more compressed from modern-day lifestyle. This opens up muscles around your shoulder — like the lats and chest — that can commonly become stiff from sitting at a computer. This movement can literally reshape the bone surrounding your shoulder to make more space in the ball and socket joint so your shoulder can move more freely.
This movement also increases your grip strength, which is one of the biggest predictors of mortality. If done correctly, it can actually make your shoulders and core stronger and more resilient, giving you more strength and athleticism throughout your entire body.
If you’re new to this exercise, you may initially hang for only a few seconds. With regular practice, you will aim to gradually increase the time spent on your regular practice of this exercise. I like to do it first thing in the morning after waking up and before I go to bed. I also integrate it into my resistance training.
General Recommendations on Duration
A good target hang time is 90 seconds for men and 60 seconds for most women. Though longer durations are possible, it’s more beneficial to aim for shorter, more frequent sessions. A total daily hang time of 3 minutes is an excellent goal.
While there’s substantial benefit in accumulating 3 minutes of dead hanging time per day, aiming for a continuous hang of 1 minute for women and 90 seconds for men, repeated twice daily for men and three times daily for women for a total of 3 minutes is a far better goal. I typically dead hang for two minutes twice a day. Seeking to work my way up to 3 minutes as a personal challenge.
The longer dead hanging time significantly enhances muscular strength in your grip and hands compared to shorter, more frequent sessions. Initially, breaking it up into smaller durations may be necessary for most people starting out. However, as you progress, you’ll find it increasingly feasible to comfortably maintain the hang for the full duration — either 1 minute for women or 90 seconds for men.
This duration should suffice for general fitness goals. Nevertheless, for those who are particularly competitive or ambitious, consider challenging yourself further by extending the time. Aim for longer holds like 2 or even 3 minutes, depending on your strength and endurance levels. That said, hanging longer than 3 minutes is unnecessary and may be counterproductive.
Recommended Setup
The dead hang is a simple exercise that requires little equipment. Here are some general tips and suggestions for getting started.
| Setting up — Use an overhead bar, like a pull-up bar, which can be easily purchased online. |
| Bar height — The bar should not be so high that you need to jump to reach it, as this could shock your shoulders. Ideally, you should be able to reach the bar on your tiptoes. |
| Using a stool or chair — If needed, use a stool or chair to help you reach the bar comfortably. |
| Exercise caution — The key precaution is to avoid straining your shoulders. |
| Performing the dead hang — Simply grab the bar with palms facing away from you and hang, keeping your body still. Hold on to the bar until your grip starts to fatigue. What you will notice is that the bar will gradually slip away from your hand grip until you can’t hold on any longer. This is a sign that you have reached your limit. For many this will be 10 to 15 seconds when starting out. |
| Progressions — To accelerate your progress, consider placing your feet down for assistance to make it to the full minute. Some may need to start with their feet down the whole time and that’s completely fine. As you build up your strength for the full 60 second hang, you can intermittently lift your toes off the support and then place them back down gradually decreasing the assistance time until you are able to dead hang for a full minute without any assistance. |
| Gradually increase your hang time — Ideally work up to a total daily hanging time of 3 minutes done over as many times as you need to get there. |
https://articles.mercola.com/sites/articles/archive/2024/03/29/dead-hang.aspx
Pineapple Enzyme Kills Cancer Without Killing You
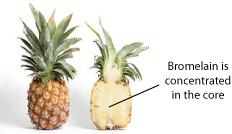
Could an extract of pineapple fruit be both safer and more effective than a blockbuster chemotherapy agent?
Every once in a while a study pops up on the National Library of Medicine’s bibliographic citation database known as MEDLINE that not only confirms the therapeutic relevance of natural substances in cancer treatment, but blows the conventional approach out of the water. Published in 2007 in the journal Planta Medica, researchers found that an enzyme extracted from pineapple stems known as bromelain was superior to the chemo-agent 5-fluorauracil in treating cancer in the animal model. The researchers stated:
This antitumoral effect [bromelain] was superior to that of 5-FU [5-fluorouracil], whose survival index was approximately 263 %, relative to the untreated control.
What is so remarkable about this research is that 5-FU has been used as a cancer treatment for nearly 40 years, and has been relatively unsuccessful due to its less than perfect selectivity at killing cancer, often killing and/or irreversibly damaging healthy cells and tissue, as well.
As a highly toxic, fluoride-bound form of the nucleic acid uracil, a normal component of RNA, the drug is supposed to work by tricking more rapidly dividing cells — which include both cancer and healthy intestinal, hair follicle, and immune cells — into taking it up, thereby inhibiting (read: poisoning) RNA replication enzymes and RNA synthesis.
Keep in mind that a 7.5 gram dose of 5-FU, which is the weight of 3 pennies, would kill 50% of the humans given it. Bromelain’s MSDS, on the other hand, states the LD50 to be 10,000 mg/kg, or the equivalent 1.5 lbs of bromelain for a 150lb adult, which means it is 3 orders of magnitude safer!
How then, can something as innocuous as the enzyme from the stem/core of a pineapple be superior to a drug that millions of cancers patients over the past 40 years have placed their hopes of recovery on, as well as exchanging billions of dollars for?
There is a well-known effect associated with a wide range of natural compounds called “selective cytotoxicity,” whereby they are able to induce programmed cell death (the graceful self-disassembly known as apoptosis) within the cancer cells, while leaving healthy cells and tissue unharmed. No FDA-approved chemotherapy drug on the market today has this indispensable property (because chemicals don’t have behave like natural compounds), which is why cancer treatment is still in the dark ages, often destroying the quality of life, and accelerating the death of those who undergo it, often unwittingly. When a person dies following conventional cancer treatment it is all too easy to “blame the victim” and simply write that patient’s cancer off as “chemo-resistant,” or “exceptionally aggressive,” when in fact the non-selective nature of the chemotoxic agent is what ultimately lead to their death.
Keep in mind that bromelain, like all natural substances, will never receive FDA drug approval. Capital, at the present time, does not flow into the development of non-patentable (i.e. non-profitable) cancer therapies, even if they work, are safe and extremely affordable. This is simply the nature of the beast. Until we compel our government to utilize our tax dollars to invest in this type of research, there will be no level playing field in cancer treatment, or any treatment offered through the conventional medical establishment, for that matter. Or, some of us may decide to take our health into our own hands, and use the research, already freely available on possible natural cancer treatment, to inform our treatment decisions without the guidance of the modern day equivalent of the “priest” of the body, the conventional oncologist, who increasingly fills the description of an “applied pharmacologist/toxicologist” – nothing more, nothing less.
© December 24th 2011 GreenMedInfo LLC. This work is reproduced and distributed with the permission of GreenMedInfo LLC. Want to learn more from GreenMedInfo? Sign up for the newsletter here www.greenmedinfo.com/greenmed/newsletter.
The WHO Is A Criminal Racketeering Organization
VAERS – 76% of Vaccine-Related Miscarriages from the Past 30 Years Occurred Once Pregnant Women Started Receiving COVID-19 Vaccines

These are alarming figures, and they are even more so when we understand what VAERS data represent. The U.S. government’s guide to VAERS states, “’Underreporting’ is one of the main limitations of passive surveillance systems, including VAERS. The term underreporting refers to the fact that VAERS receives reports for only a small fraction of actual adverse events.” Some researchers have found that less than 1% of adverse events are reported in VAERS.
So, one must keep in mind that the estimated 3,414 unborn babies who died after their mothers were vaccinated against COVID-19 and had miscarriages from December 2020 through March 2022 are probably only a small fraction of the actual number of post-vaccination spontaneous abortion “adverse events.” This number may actually be 100 times greater or more.
https://behindthefdacurtain.substack.com/p/report-48-vaers-76-percent-of-vaccine-related
Unjected
Build a profile for dating, friendships or even community and get to matching with your perfect Unjected person near or far. We have been the catalyst for countless life-changing connections, marriages and relationships.
https://unjected.com/e for dating, friendships or even community and get to matching with your perfect Unjected person near or far. We have been the catalyst for countless life-changing connections, marriages and relationships.