

Slides from an informative presentation at: https://www.youtube.com/watch?v=VA7Zvo-tzA8&list=TLGGwkRI-ZioBe0wNjEwMjAyNA&t=224s

Tom's Blog on Life and Livingness
Slides from an informative presentation at: https://www.youtube.com/watch?v=VA7Zvo-tzA8&list=TLGGwkRI-ZioBe0wNjEwMjAyNA&t=224s
A relatively recent study adds to the already impressive body of research in this field. Titled “Comparing the Therapeutic Effects of Garlic Tablet and Oral Metronidazole on Bacterial Vaginosis: A Randomized Controlled Clinical Trial,” medical researchers demonstrated the power of garlic in treating bacterial vaginosis, one of the most common gynecological infections afflicting women of reproductive age today.
Bacterial vaginosis (BV) affects 29.2% of women aged 14-49, and 25% of pregnant women in the US, according to CDC statistics. According to the study,
“This infection is asymptomatic in 50% to 75% of cases and symptomatic cases present with homogeneous gray-white vaginal discharge with fishy odor, especially after intercourse or during menstruation”
It is believed that BV results from reduced quantities of hydrogen peroxide producing lactobacillus and increased anaerobic organisms such as Gardnerella vaginalis, Mycoplasma hominis, and Prevotella species. Antibiotics are notorious for lacking specificity in inhibiting only those opportunistic strains that can cause harm, which is why it is no wonder that the standard of care treatment of BV with metronidazole has a notoriously poor success rate.[1]
Moreover, antibiotics like metronidazole come with a wide range of side effects, including nausea, diarrhea, vomiting, headache, dizziness weight loss, and abdominal pain.
Even more concerning is the fact that the drug has been identified as a potential carcinogen both by the US National Toxicology Program (NTP)[2] and the WHO International Agency for Research on Cancer.[3]
The new study tested whether garlic could compete with metronidazole in treating BV. Garlic was a logical choice, since it has been used as an anti-infective agent for millennia, and has seen a tremendous amount of clinical validation in the past ten years, as evidenced by the literature on our Garlic Research Dashboard. You can also read previous reporting we have done on the topic of garlic’s immense value in addressing infections, such as Judy Cohain’s article on “How to Treat a Vaginal Infection with a Clove of Garlic.” Much of this research also demonstrates the potent anti-cancer properties of this powerfully medicinal food.
The design of the new study involved giving two groups of 60 married women (aged 18 to 44 years) either 500 mg garlic tablets comprised of 85.42% garlic powder, or metradizole. Each dose of garlic powder contained the equivalent of 8.9-mg allein, a potent antimicrobial compound. Both drugs were taken with meals at the dose of two tablets each 12 hours for seven days.
The two different treatments were evaluated using a diagnostic criteria showing active infection known as Amsel’s criteria. Not surprisingly, garlic was found superior to metronidazole at reducing infection at 70% and 48.3%, respectively. Additionally, garlic was found to have far lower side effects.
The researchers concluded:
“This study reveals that garlic could be a suitable alternative for metronidazole in treatment of BV in those interested in herbal medicines or those affected by side effects of metronidazole.”

I’ll try to make this very short, so you can investigate yourself. There’s evil afoot and what we’re told are vaccines, aren’t anything of the sort. I’ve been researching vaccines for 25 years and I’ve watched every vaccine documentary in this list of 60 as well: https://www.jchristoff.com/blog/documentaries-that-include-100-s-of-health-professionals-warning-the-public-about-the-dangers-of-vaccination
I would simply suggest you watch maybe the first 3-5 in this list, to get a firm understanding of the lies that underpin this very obvious and dark vaccine agenda. After 25 years of research, I’ve never come across anything like what I came across yesterday. The vaccine industry biggest dirtiest secret is now out in the open.
In this first video below, we see something that’s extremely common. We see a top-level athlete (and perfectly healthy father, husband etc) completely crippled by the COVID injection. The COVID shot never qualified under any past science or medical definition, as a vaccination. This is why I never describe the COVID injection as a vaccine. Saying that (based on this new information), no vaccine has every qualified as a vaccine…..as is clearly explained farther down in this article. Basically, according to medical researcher Sasha Laytpova, you can’t vaccinate against any threat…..and yet her work exposes much more government, science and medical corruption than just this one bombshell revelation.
https://www.jchristoff.com/blog/the-hidden-and-ancient-vaxseen-agenda
Throughout history, many different types of intelligence have been recognized (e.g., physical intelligence and coordination or emotional intelligence). In contrast, our society worships a very specific type of intellectual intelligence that as far as I know has never previously been so highly valued by a society.
In my own experience, I’ve lost count of how many people I’ve interacted with who I know are much smarter than me (as they can do things I simply can’t), yet when I compare and contrast our ability to get things done, to correctly interpret the data we are exposed to, help patients, or the general capacity to lead a happy life, I come out far ahead of them. Likewise, I’ve lost count of how smart people I’ve met who simply don’t “get it” and frequently are misled by something quite obvious—an experience I am sure many of you can relate to.
Keep reading: https://www.midwesterndoctor.com/p/the-importance-of-balanced-intelligence
Of course, while the science is starting to catch up, and the lawsuits are continuing apace (source), we’re still being told by our governments and mainstream media to roll up our sleeves, even those of us as young as 6 months.
https://okaythennews.substack.com/p/covid-vaccine-science-catching-up
It is also known as E102, FD&C and Yellow 5.
Watch: https://www.armstrongeconomics.com/world-news/corruption/tartrazine-make-america-healthy-again/
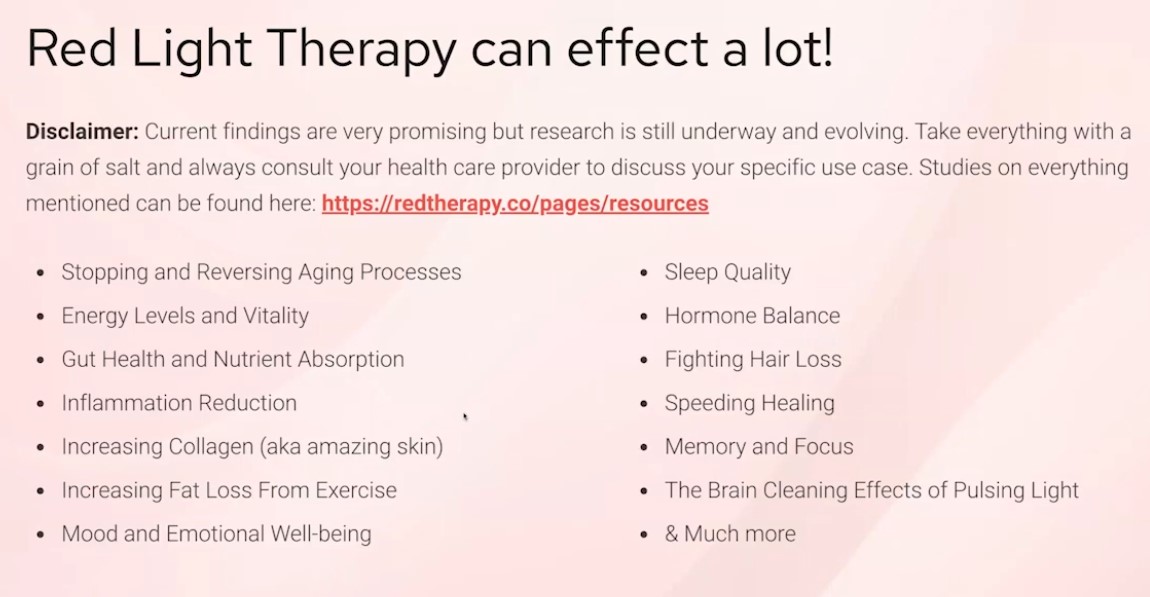
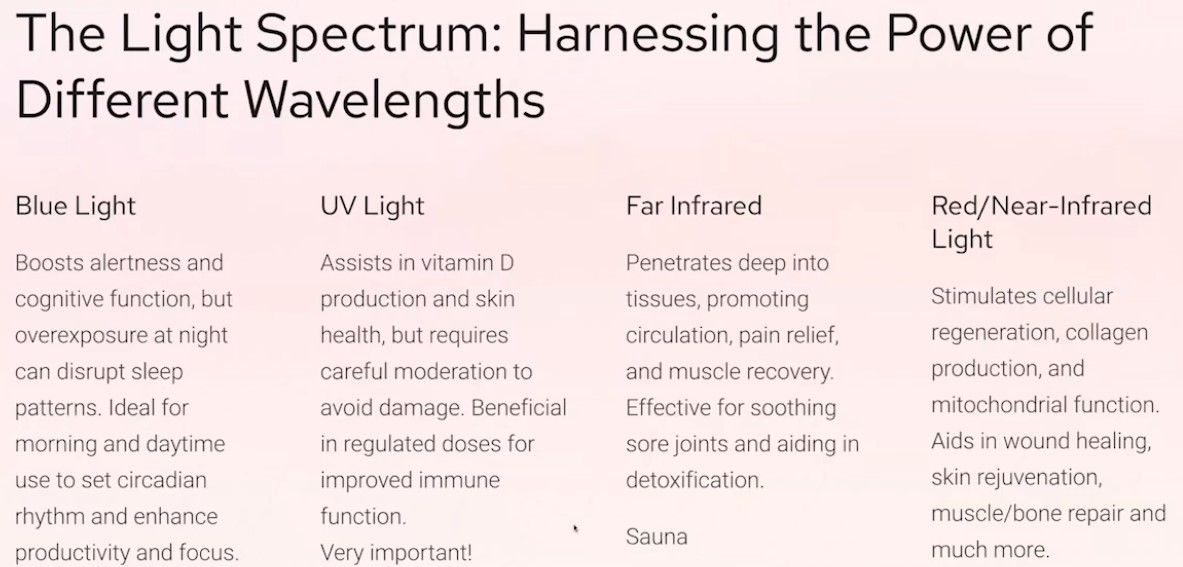
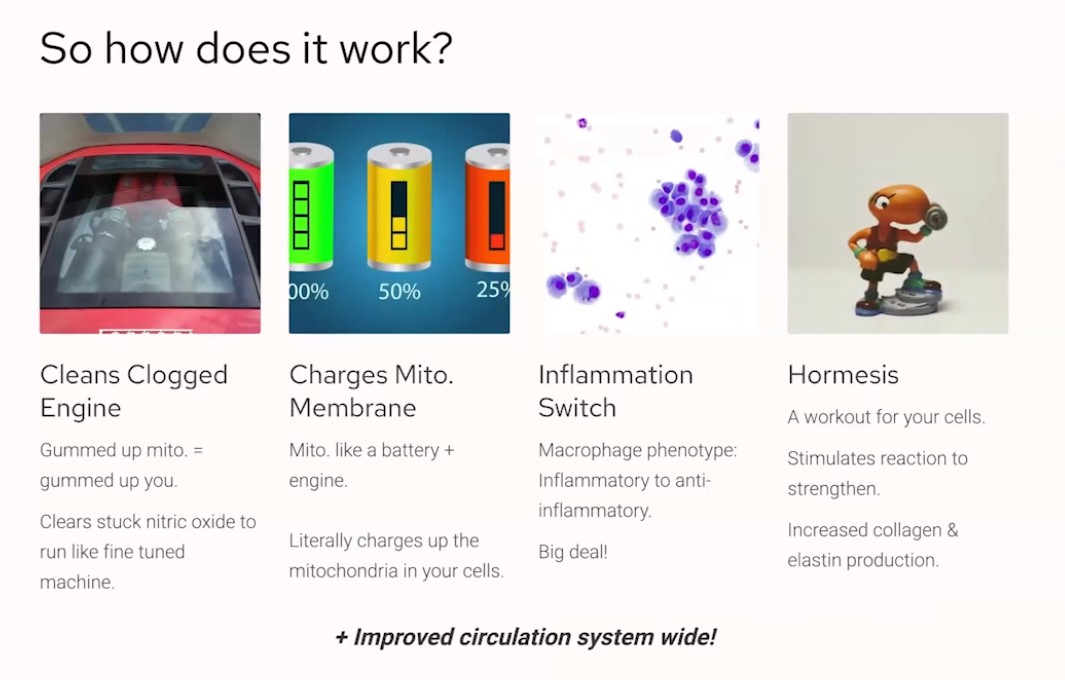
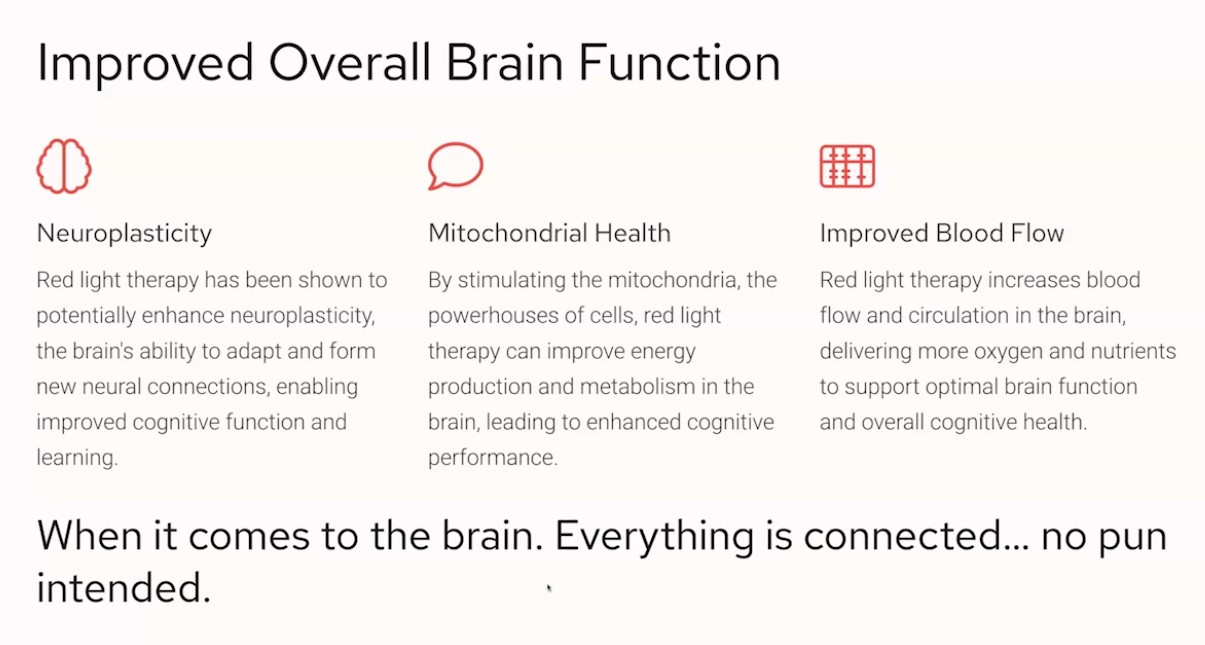
I have been watching the presentations in the ageless summit. Here is some interesting data on red light therapy from one presenter.

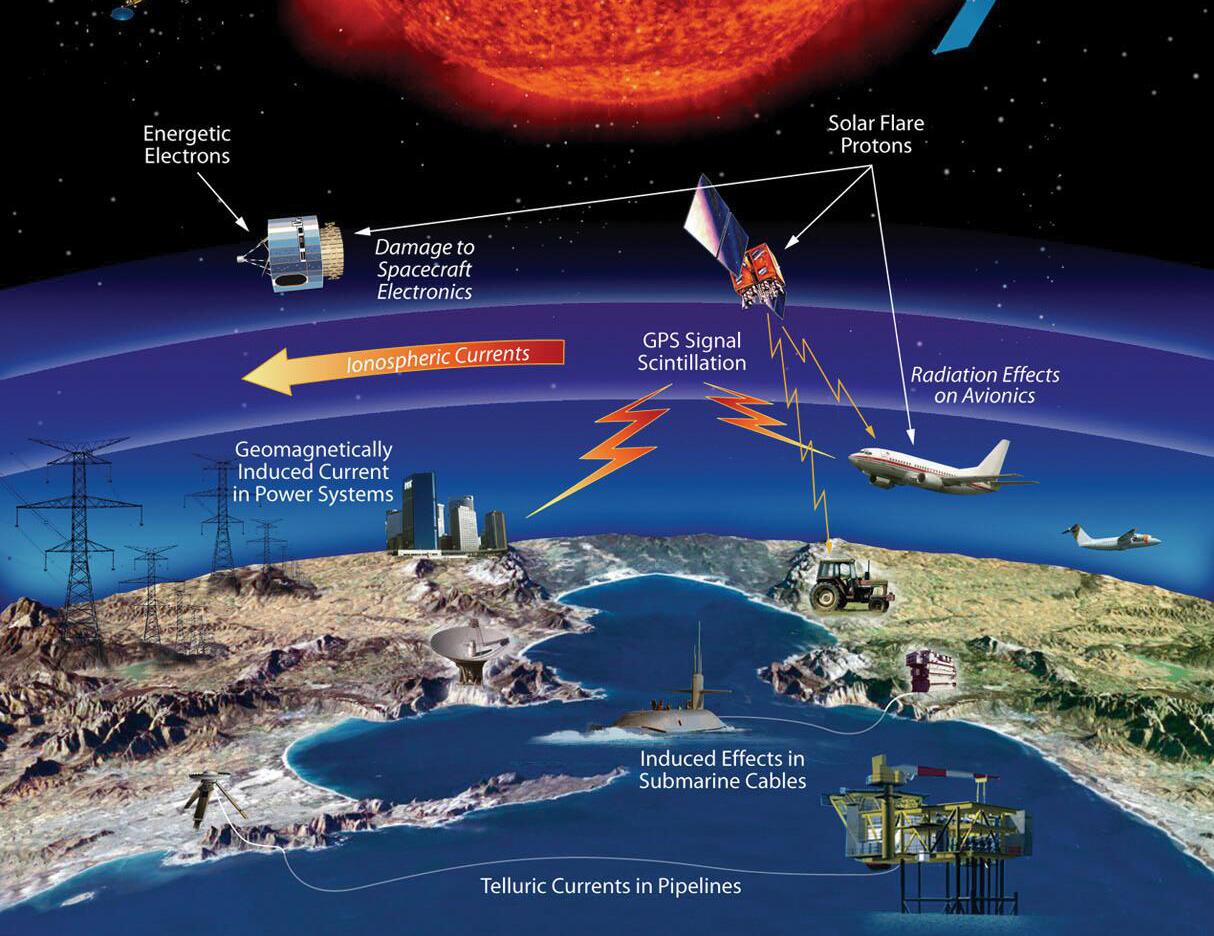
“Today’s incredible X9.0-class solar flare, the most intense flare since 2017. An Earth-directed solar storm is highly likely, given the spot region is faced directly at Earth,” Space Weather Watch wrote on X.
Keith Scott-Mumby writes:
After 30 years, the truth is now known—Eli Lilly, the makers of Prozac, secretly paid off plaintiffs in a court case following a mass shooting incident. Prozac was and is the number one deadly type of drug that sends people crazy and triggers aggression and murderous violence. It was known to do so by the FDA when the drug was first reviewed.
That agency went rogue a long, long time ago. It takes no responsibility for launching killer chemicals on the population. In fact, the original FDA examiner said NO to the drug: it caused aggression and violence. He knew that. But he was overruled. The drug came to the market anyway.
The plaintiffs suing Eli Lilly were families of the victims of Joseph Wesbecker, a man who went on a deadly shooting rampage in Louisville, Kentucky. He killed 8 and injured 12. It was a critical moment in the history of these drugs because they had been reported to cause violence. If Eli Lilly lost the case, that could be the end of a marvelous gravy train for the industry (as of this writing, 1 in 5 US citizens are on some form of psychiatric medication).
But the trial was rigged. Eli Lilly was exonerated at the time, absolved of any blame for murders by the jury. But it was not an honest trial. Eli Lilly shamelessly (and criminally) gave $20 million in secret bribes to
potential witnesses in another trial, which could have gone badly for them at the critical moment.
Not only was Eli Lilly bailed out and escaped consequences. The drug too was “exonerated” and now it’s difficult to get the bent psychiatric profession to tolerate the idea that their stupid drugs are causing mass murders. Prozac and other SSRIs KILL people.
Eli Lilly vigorously shielded the illegal and corrupt payment for more than two decades, defying the Louisville judge who fought to reveal it because he said it swayed the Wesbecker jury’s verdict.
That heroic judge, Circuit Judge John Potter, suspected that Lilly bribed plaintiffs and their lawyers before the jury verdict. He uncovered evidence of bribery, and fought Eli Lilly for years but failed to obtain adequate proof of the terms of the Prozac payoff deal. Lilly succeeded in keeping its criminal action from a judicial proceeding.
As is Big Pharma’s usual strategy, they also trashed the judge and ruined his life, for his pursuit of the truth (Jon Rappoport. www.nomorefakenews.com).
Who Is The Victim Here, The Killer?
On Sept. 14, 1989, Joseph Wesbecker entered a Louisville print shop around 8:30 a.m., carrying a bag full of weapons, including a semiautomatic rifle. Over the next 30 minutes, as he walked through the building, Wesbecker fired more than 40 rounds at those he encountered before shooting himself in the [head] with a handgun.
So the “official” story is he was crazy. That’s why he committed the murders. But Wesbecker had no murderous traits or suicidal till he started taking Prozac a month before. Moreover, this was far from a one-off. Scores of mass murders have now been committed by individuals driven mad by psychiatric drugs.
But the call is now for more drugs, to dose more patients, because they are crazy and might do harm. They are now even subjecting kids at school to psychiatric tests, to see if they have any “tendencies”. If any are spotted, they are put on psych meds. That’s why so many mass murderers are mere kids of school-age (Sandy Hook, Columbine, Parkland… look ’em up).
Jon Rappoport has done a sterling job in collecting media critiques of these deadly drugs:
On February 7th, 1991, Amy Marcus’ Wall Street Journal article on the drug carried the headline, “Murder Trials Introduce Prozac Defense.” She wrote, “A spate of murder trials in which defendants claim they became violent when they took the antidepressant Prozac are imposing new problems for the drug’s maker, Eli Lilly and Co.”
Also on February 7, 1991, the New York Times ran a Prozac piece headlined, “Suicidal Behavior Tied Again to Drug: Does Antidepressant Prompt Violence?”
In his landmark book, Toxic Psychiatry, Dr. Breggin mentions that the Donahue TV show (Feb. 28, 1991) “put together a group of individuals who had become compulsively self-destructive and murderous after taking Prozac and the clamorous telephone and audience response confirmed the problem.”
Breggin also cites a troubling study from the February 1990 American Journal of Psychiatry (Teicher et al, v.147:207-210) which reports on “six depressed patients, previously free of recent suicidal ideation, who developed an intense, violent suicidal preoccupation after 2-7 weeks of fluoxetine [Prozac] treatment. The suicidal preoccupations lasted from three days to three months after termination of the treatment. The report estimates that 3.5 percent of Prozac users were at risk.
While denying the validity of the study (of course), Dista Products, a division of Eli Lilly, put out a brochure for doctors dated August 31, 1990, stating that it was adding ‘suicidal ideation’ to the adverse events section of its Prozac product information.”
An earlier study, from September 1989 Journal of Clinical Psychiatry, by Joseph Lipiniski, Jr., indicates that, in five examined cases, people on Prozac developed what is called akathisia. Symptoms include intense anxiety, inability to sleep, the “jerking of extremities,” and “bicycling in bed or just turning around and around.”
Breggin comments that akathisia “may also contribute to the drug’s tendency to cause self-destructive or violent tendencies … Akathisia
can become the equivalent of biochemical torture and could possibly tip someone over the edge into self-destructive or violent behavior … The June 1990 Health Newsletter, produced by the Public Citizen Research
Group, reports, ‘Akathisia, or symptoms of restlessness, constant pacing, purposeless movements of the feet and legs, may occur in
10-25 percent of patients on Prozac.”
There are other studies: “Emergence of self-destructive phenomena in children and adolescents during fluoxetine [Prozac] treatment,” published in the Journal of the American Academy of Child and Adolescent Psychiatry (1991, vol.30), written by RA King, RA Riddle, et al. It reports self-destructive phenomena in 14% (6/42) of children and adolescents (10-17 years old) who had treatment with fluoxetine (Prozac) for obsessive-compulsive disorder.
The Journal of the American Academy of Child and Adolescent Psychiatry, September 1991. Author Laurence Jerome reports the case of a ten-year-old who moves with his family to a new location. Becoming depressed, the boy is put on Prozac by a doctor. The boy is then “hyperactive, agitated … irritable.” Then he calls a stranger on the phone and says he is going to kill him. The Prozac is stopped, and the aggressive symptoms disappear. And Jon Rappoport (www.nomorefakenews.com) reminds us that what is true about Prozac is true about Paxil or Zoloft or any of the other SSRI antidepressants.
Why Am I Telling You This?
Because psychiatry is about the last word in mindless, dangerous, fake, criminal, unscientific meddling with the human mind. It is a million miles from the true science and medicine of the mind. IT IS BUT A TOOL IN THE HANDS OF THE CRAZY PHARMA CRIMINALS, who would like to see EVERYONE dosed on chemical toxins, to shut us up, make us docile and willing to accept the coming world-order control of mass populations.
The psychiatric profession (as a whole, not individuals like Peter Breggin and my friend Clancy McKenzie) makes George Orwell’s 1984 scenario seem like an enjoyable vacation. The population is systematically being doped to extinction.
PSYCHIATRY HAS NO SCIENCE, NO METHOD. It just throws deadly drugs at the problem and hopes that something will stick. And it is winning hands down in this strategy because psychiatric drugs CAUSE mental illness! I’ll write that again: PSYCHIATRIC DRUGS CAUSE MENTAL ILLNESS.
The more drugs they sell, the more customers they get (for life).