
Dr David E Martin On Remdesivir

“Remdesivir was declared too deadly & unethical to use In African Ebola Trials because it had a 53% kill rate.” ~Dr David E Martin
It was the only drug Fauci allowed to be used on COVID patients in Hospitals.
Families whose loved ones were killed call it ‘Run-Death-Is-Near.’..
Remdesivir kills kidney function, combine that with a ventilator & patients develop Pulmonary Edema, causing their lungs to fill with fluid & drown to death.
Remdesivir kills the liver & causes multi organ shut down.
In the halted Ebola trial, Remdesivir mortality was 53% overall & 85% mortality in those with high viral load.
Anthony Fauci claimed that Remdesivir would stop Covid; instead, it stopped kidney function, then blasted the liver & other organs.
• 2.81X KIDNEY FAILURE RISK—permanent damage in patients.
• HEART DAMAGE: Triggers fatal arrhythmias, cardiac arrest, & bradycardia.
• LIVER INJURY: Causes severe, irreversible hepatocyte damage.
• INFANT APPROVED: Now FDA-approved for NEWBORNS at birth as long as they weigh 3 lbs—tested on just 58 infants for 10 DAYS!
Click to view the video: https://x.com/ValerieAnne1970/status/2076305581594591272?s=20
Essential Oils For Sleeping
Researchers at the University of California, Irvine (UCI) conducted a groundbreaking 6-month study on how olfactory stimulation during sleep can dramatically boost memory and cognitive capacity.
Participants in the experimental group used an odorant diffuser in their bedrooms for two hours each night. Rather than using a single scent, they were exposed to a daily rotation of seven essential oils: rose, orange, eucalyptus, lemon, peppermint, rosemary and lavender. The researchers emphasized that this daily rotation—to ensure novelty—is vital for supporting neuroplasticity.
Compared to a control group that diffused distilled water, the olfactory-enriched group demonstrated a remarkable 226% improvement in cognitive capacity. The significant cognitive enhancement was primarily verified via neuropsychological word list tests.
Furthermore, MRI brain imaging revealed structural improvements in the left uncinate fasciculus, a key white matter tract connecting the brain’s memory and decision making centers.
IT IS IMPORTANT TO NOTE THAT THE ONLY OIL THAT CAN BE DIFFUSED AROUND CATS OR DOGS IN THIS LIST IS THE ROSE ESSENTIAL OIL. KEEP YOUR BEDROOM DOOR CLOSED AND PETS OUT WHEN USING THE OTHER 6 OILS LISTED IF YOU HAVE ANIMALS.
SEE PMID: 37554295
Henry Ford Vaxxed vs Unvaxxed Study
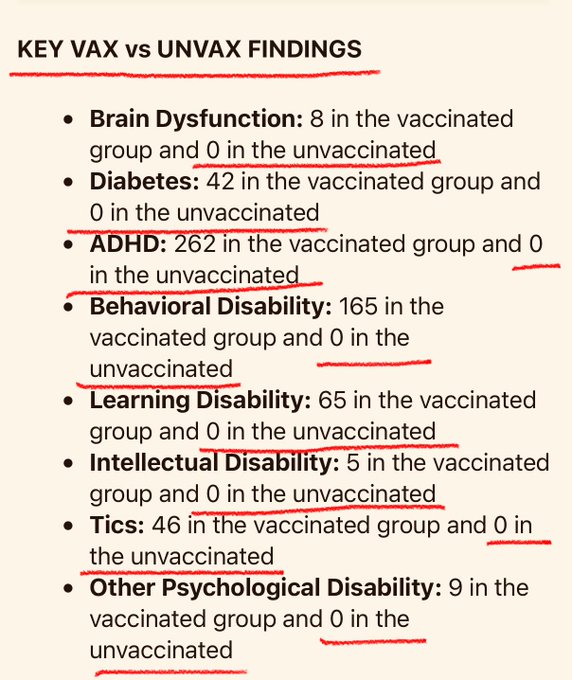
The Henry Ford Vax vs. Unvax Study with over 18,000 children was so damning that the pro vaccine researchers refused to publish it due to backlash concerns. Now you know why…
WA Covid Jab Data
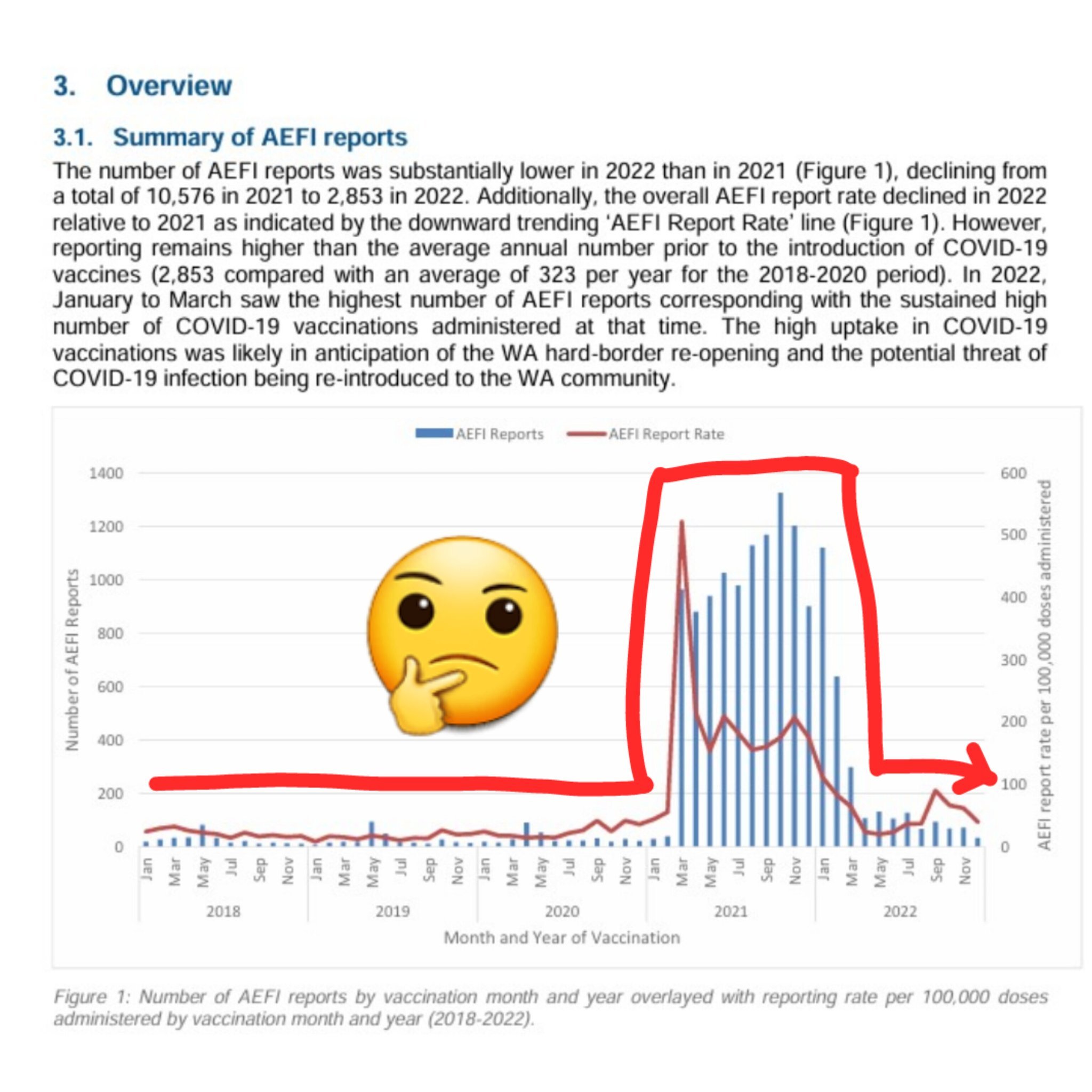
Western Australia accidentally conducted one of the world’s largest real-world vaccine safety experiments.
From April 2020 until March 2022, Western Australian was isolated from the rest of Australia and the world. Its borders were closed, and for almost two years there was virtually no community transmission of COVID-19.
That makes Western Australia’s data unique.
Across 2020 and 2021, a population of around 2.7 million people recorded just 1,223 COVID-19 cases. Some of which were classified as ‘historical cases’, and only around 11% were acquired locally. Most cases were linked to international arrivals, known contacts, or existing cases/clusters.
By the end of 2021, almost 4.1 million COVID-19 vaccine doses had been administered in the state.
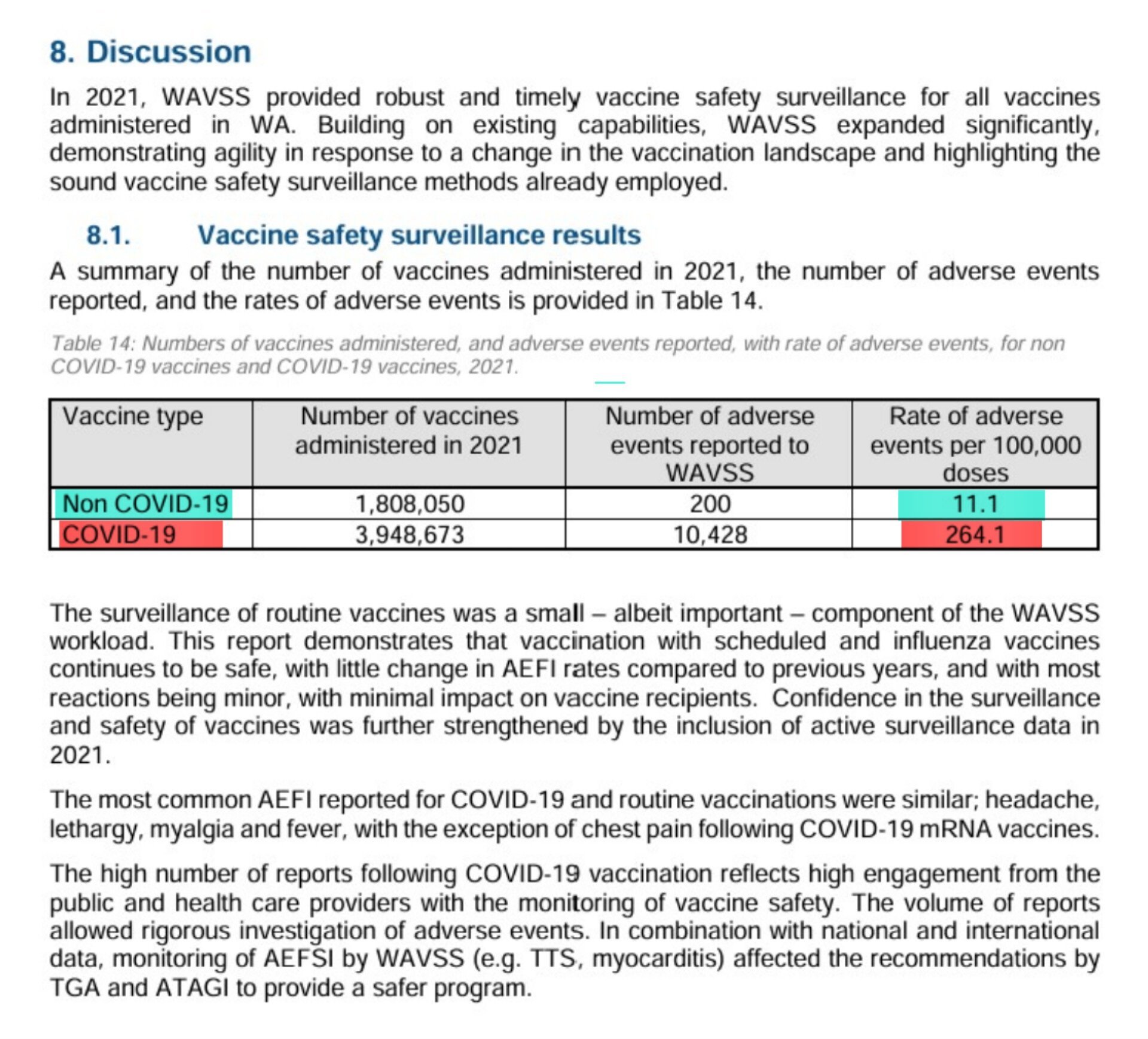
According to the Western Australian Vaccine Safety Surveillance Annual Report 2021, the reported adverse event rate for all non-COVID vaccines was 11.1 per 100,000 doses.
For COVID-19 vaccines, it was 264.1 per 100,000 doses.
That is a reported adverse event rate per dose approximately 23.8 times higher than for all other vaccines combined.
Those figures deserve attention.
Western Australia’s experience was unlike almost anywhere else on Earth.
Millions of vaccine doses administered in a population with very limited exposure to the virus and a material spike in adverse events.
If we are to learn from history, this data deserves our attention.
Finish reading: https://x.com/arbsmichael/status/2076579197875552760?s=20
Antarctica Is Not Warming, It Is Freezing
Antarctica is colder and more icebound today than at any point in the past 5,000 years.
Research by Hall (2023) found that West Antarctica cooled by more than 1.8C between 1999 and 2018.
Satellite data confirm continent-wide cooling, as do multiple glacier studies.
View the video: https://x.com/Electroversenet/status/2076396177914753107?s=20
Bastian Obermayer – Interested In Data?

It began with four words from a stranger. John Doe.
No name. No face. Just a message on an encrypted screen in the middle of the night. “Hello. Interested in data?” Then a warning that would have made most people close the laptop and walk away. “My life is in danger. We can never meet.”
The reporter said yes. And a ghost handed him the biggest secret in the world.
Bastian Obermayer was a journalist in Germany. He chased the stories nobody else would touch. That night, the files started to arrive. First a trickle. Then a flood.
They came from a law firm in Panama. Mossack Fonseca. Most people had never heard of it. But it was one of the most powerful secret-keepers on Earth.
The firm built shell companies. Empty shells on paper, designed to hide who really owned the money. If you were rich and wanted a fortune to disappear, this is where you went. No questions asked.
And John Doe was handing all of it to a reporter.
11.5 million documents. Emails. Passports. Bank records. Forty years of buried secrets. It was the biggest leak in the history of journalism. Nothing had ever come close.
Obermayer showed his colleague, Frederik Obermaier. The two of them stared at the screen. And they understood something immediately.
This was too big. Too big for two men. Too big for one newspaper. Too big for one country.
So they did something almost no journalist ever does. They gave it away.
They took it to the ICIJ, a global network of investigative reporters. And together they built the impossible — the largest reporting team in history.
Around 400 journalists. Over 100 news outlets. Nearly 80 countries. 25 languages. All working the same secret, at the same time, for more than a year.
And not one of them leaked it.
Stop and think about that. Four hundred journalists. A year of silence. The story of a lifetime sitting in their hands. And they waited. Because if a single word slipped out early, the powerful would bury it under lawyers, threats — maybe worse.
Then they dug in. And what they found was staggering.
The secret money of the most powerful people alive. 140 politicians. World leaders. Kings. Billionaires. Drug dealers. Arms dealers.
A $2 billion trail leading to the inner circle of Vladimir Putin. The cousin of a brutal dictator. The families of sitting prime ministers.
And here is the detail that tells you how untouchable they felt. They hid their fortunes in shell companies with childish code names. One was called Harry Potter. One was called Winnie the Pooh.
The entire hidden world of the ultra-rich. Mapped out. In black and white.
And here is why it should make your blood boil. That money didn't vanish into thin air. It was tax that never got paid. The money that should have built your schools, your hospitals, your roads — quietly funneled offshore by the richest people on the planet, while you paid every cent of yours.
April 3, 2016. The day arrived. Around the world, at the very same moment, the stories went live.
The Panama Papers.
The earth shook.
Within days, the Prime Minister of Iceland resigned. Crowds had flooded the streets. He was finished. Pakistan's Prime Minister was thrown out of office too. The leak chased leaders across the planet.
Police raided offices. Governments opened more than 150 investigations across 79 countries. Over a billion dollars in hidden taxes was clawed back, country after country. New laws were written. The secret world was dragged into the daylight.
And the firm at the center of it all, Mossack Fonseca, collapsed. It shut its doors forever. Its founders were arrested.
But there was a cost. A terrible one.
A journalist in Malta named Daphne Caruana Galizia chased the offshore secrets in her own country. She would not stop. In 2017, a bomb was planted in her car. She was killed. Murdered for the truth.
The reporters carried that with them. They always knew the danger was real.
And the ghost? John Doe? The one who started it all?
He was never found.
He stayed hidden — even from the reporters he handed everything to. They never learned his name. They never saw his face. He gave the world its biggest secret, and asked for nothing in return.
Think about what they all did.
Two reporters got the call of a lifetime. They could have kept it — the glory, the prizes, all for themselves. Instead they shared it with 400 strangers and trusted the whole world to carry it together.
They took on presidents, kings, criminals, and the richest people on Earth. With nothing but documents and nerve.
And they won. They won the Pulitzer Prize — the highest honor in journalism. They even made a film about it. Meryl Streep starred in it.
The shell companies are harder to hide behind now. The laws are stronger. The powerful are a little more afraid. All because of one leak from one stranger who refused to give their name.
And John Doe is still out there somewhere. Still hidden. Still safe, the reporters hope.
Somewhere in the world is a person who gambled their life to hand humanity the truth — and never once asked for thanks. The only reward they'll ever receive is being remembered.
So don't let this one scroll quietly past. Some secrets were bled for.
Tag someone who still thinks the rich play by the same rules you do.
Quote of the Day
“Honesty is the first chapter in the book of wisdom.”
Thomas Jefferson (1743-1826) Principal author of the Declaration of Independence, 3rd President of the United States (from 1801 to 1809)
How language shapes the way we think

(Tom: Interesting. So English natively teaches us to be more responsible for the results of our actions.)
There are about 7,000 languages spoken around the world — and they all have different sounds, vocabularies and structures. But do they shape the way we think? Cognitive scientist Lera Boroditsky shares examples of language — from an Aboriginal community in Australia that uses cardinal directions instead of left and right to the multiple words for blue in Russian — that suggest the answer is a resounding yes. “The beauty of linguistic diversity is that it reveals to us just how ingenious and how flexible the human mind is,” Boroditsky says. “Human minds have invented not one cognitive universe, but 7,000.”
Click to view the video: http://t.ted.com/8xlhL9i
EPWC Presentation

First hand reports of efforts to suppress the temperature truth to support the man-made global warming lie.
View video: https://x.com/FatEmperor/status/2076037263188758847?s=20