MIT biologist says fear mongering on coronavirus will go down as biggest fraud to manipulate economies
(Tom: This is yet another of the “dissenting voices” that promte the building up of the natural defences of the human body rather than relying on an ever increasing array of toxic drugs, each designed to combat a single menace. Life evolves to assume different forms better equipped to counter threats to its survival. That’s why we hear that the COVID-19 has already morphed twice into a new form. That’s why each year’s flu shot is less than 10% effective – because it is combatting a morphing enemy. Do yourself a favour and opt out of the drug company/medico paradigm and research the subject until you fully duplicate how the body works in response to pathogens then, and most importantly, alter your nutrient intake, exercise regime, sleep patterns and stress levels until you are closer to an optimally functioning human being.)
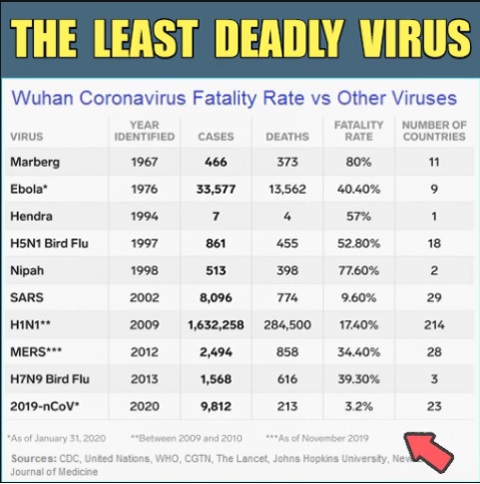
On March 11, the World Health Organization (WHO) declared COVID-19 a global epidemic. The virus, which originated from Whuan China, has claimed over 4,000 lives with 100,000 infected cases reported worldwide. However, some think the panic over the coronavirus is overblown and could potentially do more damage to citizens and overburden our already fragile healthcare systems.
Dr. Shiva Ayyadurai, an MIT scientist and researcher on the human immune system, is one the most respected experts who think the media and the “Deep State” are doing the world a disservice by exaggerating the impact of the virus. He said it’s time to stop scaring people and start talking about immune health.