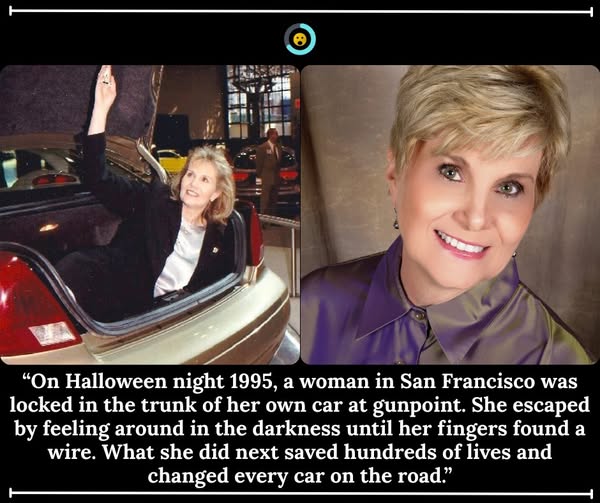
Her name was Janette Fennell. And she was 41 years old when it happened.
Janette had spent her career as a marketing and sales executive in San Francisco – sharp, driven, the kind of person who understood how systems worked and how to move people. In 1995, she had taken a break from all of that to raise her firstborn son, Alex. He was 9 months old.
He had been wearing a pumpkin outfit that night because it was Halloween.
29 October 1995. San Francisco. Just before midnight.
Janette and her husband pull into the garage of their home after dinner at a friend’s house. Alex is asleep in the backseat. The night is ordinary in every way.
Then 2 men in Halloween masks come out of the dark, and they are holding guns.
In the space of seconds, the Fennells are forced out of the car and into the trunk. She hears the lid close. She hears the engine start. She does not know where her son is.
The car backs out of the garage and drives into the night.
In the trunk, in complete darkness, Janette Fennell does something remarkable. She does not panic — or rather, she panics and keeps moving anyway. She and her husband run their hands along every surface of the trunk, searching for anything that could help them. At some point, her fingers find a gap in the interior lining. Behind it, a thin cable. A faint line of light from somewhere in the car’s mechanics.
She pulls it.
Nothing.
She keeps feeling. She keeps looking for the light.
They are driven through the streets of San Francisco and out into the darkness beyond. At some point the car stops. The men open the trunk. They assault the Fennells, take what they want, and leave them there – in the trunk of their own car, at a remote location, with no idea whether their infant son is alive.
Eventually, somehow, the Fennells claw their way out. They make their way back. Alex had been removed from the backseat by the men and placed in the foyer of their home, unharmed, before the car drove away.
They were all alive.
And Janette Fennell, who had just spent hours in a locked car trunk in the dark, now knew something that most people in America did not, there is no way out.
The problem, as Janette sees it, is an engineering problem.
Every car trunk built in America is constructed from the outside in – a mechanism designed entirely to keep the lid closed. There is a latch, operated by a key or a button. There is no corresponding mechanism on the inside. Nothing to pull, nothing to push. If you are in the trunk, you are in the trunk, and the only way you are getting out is if someone opens it from outside.
This is not controversial. This is simply how cars are built. It has never occurred to the automotive industry that it needed to be otherwise.
Janette goes to the car manufacturers and explains the problem. They listen politely. They tell her that trunk entrapment is vanishingly rare, that the data doesn’t support a mandate for redesign, that the cost would be significant for a risk that is statistically minimal.
She goes back.
She starts gathering data.
She founds an organisation called TRUNC – the Trunk Releases Urgently Needed Coalition — and begins building the evidence base that the automakers say doesn’t exist. She combs through death records, police reports, emergency service calls. She tracks cases of adults locked in trunks by criminals. She tracks the cases no one wants to talk about: children.
Because here is what Janette has come to understand. It is not only kidnapping victims who end up trapped in trunks. Every summer in America, children – curious, playful, unsupervised for a moment – climb into car boots and pull the lid shut behind them. On a cool day, a child locked in a trunk might be uncomfortable and frightened. On a hot day, in the middle of summer, a car trunk becomes an oven in minutes. Core body temperature rises. Organs begin to fail.
The children who die this way die slowly, in the dark, alone.
Janette takes her data to Congress.
The late 1990s. Washington, D.C.
She finds an ally in Representative Bart Stupak of Michigan, who is persuaded by the evidence and sponsors a bill to require the National Highway Traffic Safety Administration to study the problem formally. NHTSA forms an expert panel. Janette is on it.
Then, in the summer of 1998, everything changes.
A 3-week heatwave settles over the United States. In the space of those 3 weeks, 11 children die locked in car trunks. It is an avalanche of preventable deaths, concentrated into less than a month, and it is impossible to look away from.
The automotive industry still resists. They argue that criminals could simply disable an internal release mechanism. They argue that the data doesn’t support the cost. They argue, and Janette keeps showing up, and the children keep dying, and she keeps showing up again.
She testifies before committees. She meets with executives. She brings the families of children who did not survive. She is precise, factual, relentless – the way a person is relentless when they have been inside the thing they are asking people to take seriously.
1 September 2001.
The National Highway Traffic Safety Administration issues its mandate. Every new passenger car manufactured with a trunk must be equipped with an internal release mechanism – operable from inside the trunk – as standard equipment.
The mechanism must glow in the dark. So that a child in the dark, in the heat, with no understanding of what is happening to them, can find it.
Every car built in America from model year 2002 onward has a small luminescent handle inside the trunk. It is usually yellow or green. Most people have never noticed it. Many people don’t know it exists.
Janette Fennell knows it exists. She put it there.
After the trunk mandate, she went on to found Kids and Car Safety – a national organisation dedicated to preventing every kind of harm to children in and around vehicles. She has spent the decades since tracking heatstroke deaths, backover incidents, power window entrapments. She has never stopped showing up.
In her 2003 Senate testimony, she said simply- “We were able to use this traumatic experience to help guide the Federal Regulatory process to ensure that no one else had to end up in the trunk of a vehicle without a way to escape.”
The next time you open your car boot and see the small glowing handle in the corner, you are looking at 1 woman’s answer to the worst night of her life.
Share this with someone who needs to be reminded what it looks like to turn something terrible into something that protects the people who come after you.