
Who Needs Flowers?
I found this delightful story online and want to share it. It’s from a woman in California: My husband did not want children, DID NOT WANT. I couldn’t have children. A marriage made in heaven. About three years into the marriage, my brother and his wife were killed, leaving a toddler and an infant. I spent the next four days comforting my parents, making funeral arrangements and planning a funeral. My husband spent those four days dealing with the fact that there were two kids that were looking at foster care. He tried to find a way out of the situation. He didn’t want to be a parent. DID NOT WANT. We never discussed the kids because we were dealing with arrangements. We were driving back to my parents’ house after the funeral and he essentially said “So we are going to be parents.” I was shocked, the fate of the kids had never come up. My response was something like “But you don’t want kids.” His response was “I love you, you would not be happy if the kids went to foster care, I want you to be happy, I will do anything for you to be happy.” To be honest, I was almost as grudging as he was, because we had plans and they didn’t include children. But he was right, I wouldn’t be happy if the kids were raised in foster care. So we became parents. Two years later we adopted both kids. My husband—who didn’t want children—spent the next roughly 18 years as the best and most devoted father I have ever met. When the kids were about seven and nine, one day I asked him why he had been so hands-on and devoted. His response was “It is a gift to you— at least it started out that way. Now I love them for themselves.” It blew my mind that he gave up or delayed his dreams and plans just to make me happy and that he did so without sulking without complaining. He was patient, devoted and kind to the children and he did it as a gift to me. Who the hell needs presents, flowers or candlelit dinners?
Frog And Mouse

Planned Food Shortages
These are not coincidences.
If you have not been laying in supplies before now you are behind the early movers, catch up while you can!
Ships Awaiting Unloading Shanghai

No reason for supply chain shortages… …looks to me like a disaster waiting to happen!
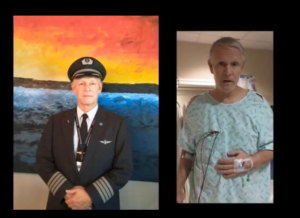
Vaccinated American Airlines Pilot Went Into Cardiac Arrest Six Minutes After Landing Commercial Flight With Nearly 200 Passengers
And here’s something you won’t hear on the main stream news outlets…
“On April 9, 2022 American Airlines Captain Robert Snow experienced a severe post-vaccination cardiac arrest inside the cockpit of Airbus 321 carrying nearly two hundred souls,” Horowitz tweeted.
The event took place at the gate six minutes after landing. This near miss is a direct result of the Federal Aviation Administration (FAA) overlooking their own safety regulations for brazenly political purposes relating to the dangerous COVID-19 vaccine mandate policies.
A group of lawyers and doctors familiar with health care protocols in civilian and military aviation in December sent a letter to the FAA and CEOs of all major airlines with a dire warning about vaccinated pilots.
According to the team of legal and medical professionals, pilots are prohibited from flying after taking a non-FDA-approved treatment or one that was approved under 12 months ago.
The Universal Antidote – The Science and Story of Chlorine Dioxide
This is a very well done documentary that explains the history, the nature and effectiveness of yet another useful wellness product the pharma funded media and controlled interests love to denigrate.
The Difference Between Knowledge And Understanding
Another piece of the jigsaw puzzle of life drops neatly into its place:
“Learning does not make one learned: there are those who have knowledge and those who have understanding. The first requires memory and the second philosophy.” – Alexandre Dumas
Fallen Leaves
With the depletion of the earth’s topsoil this is a very worth while change!
Dutch Journalist In Donbas: ‘Western Media Is Lying About What Is Happening in Ukraine’

Sonja van den Ende says the Western media “lie continuously about everything just to implement their own agenda.”