Click to view the video: https://www.youtube.com/watch?v=82-Ae8fK7iY

Tom's Blog on Life and Livingness
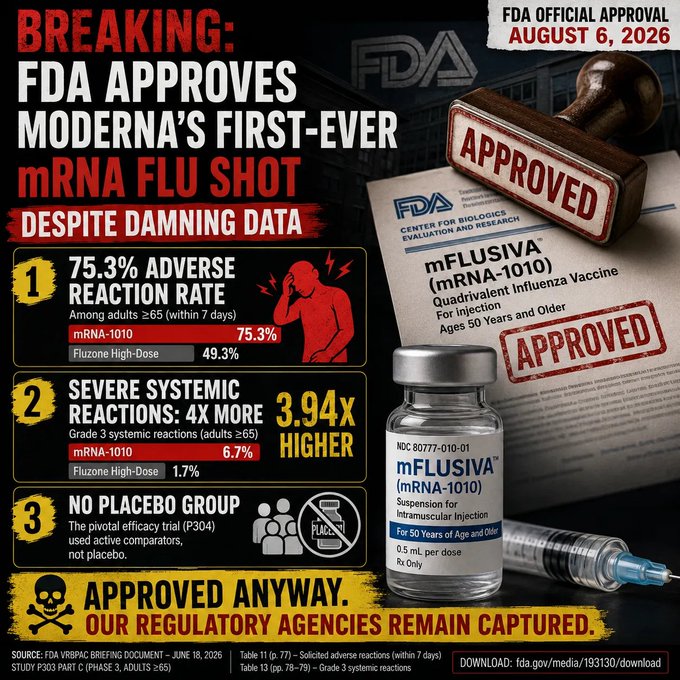
Pharma finished recapturing the Food & Drug Administration as the FDA okayed Moderna’s mRNA flu jab, which Moderna’s OWN studies show causes 270 severe side effects to stop ONE flu hospitalization.
Drug industry reform dies in darkness.
Last night, the Food & Drug Administration quietly approved Moderna’s mRNA flu “vaccine.” Moderna put out its press release at 10:15 p.m. Eastern, presumably in an effort to contain the blowback the FDA will face from MAHA and drug industry skeptics over its decision to roll over and approve this jab. Of course, legacy media outlets were ready with stories; no doubt they were tipped in advance and had pieces waiting.
As I wrote in May, the risk-benefit ratio of the jab is almost absurdly bad, based on Moderna’s own studies — which likely understate it, since drug companies will do everything they can not to connect the side effects they see in clinical trials. To quote that piece (which you can read fully below):
In other words, Moderna’s own data show that about 270 people will suffer severe vaccine side effects from its shot to stop a single flu hospitalization. In what world does that risk ratio make sense?
In a world where Moderna and Blackstone have a direct line to the White House. There was no chance the FDA would say no to this jab once the Trump Administration forced Dr. Vinay Prasad to resign from the agency in March.
The only question is whether Moderna will be able to bribe offer completely legal financial incentives to enough pharmacy benefit managers to get this new jab — which will no doubt cost far more than traditional flu shots — into the system and the arms of unwitting patients.
I’m sure benefits managers will stand up for patients and say no to a more expensive drug with worse side effects even if Moderna kicks back mucho dinero —
I’m sorry, I was laughing too hard to finish that last sentence.
Another great day for American medicine!
https://alexberenson.substack.com/p/the-moderna-flu-jab-has-a-comically

She was thirteen years old when she talked her parents into buying her a guitar. Full of excitement, she signed up for lessons — and quit after exactly one.
Because her instructor had looked at her and told her, flatly, that girls can’t play rock and roll.
She decided, right then, that he was wrong. And she set out to prove it in a way that would change music forever…
Her name was Joan Marie Larkin — though the world would come to know her by a name she took after her parents divorced, a name that fit her like a leather jacket: Joan Jett.
She’d walked out of that one and only guitar lesson and taught herself to play instead. And when her family moved out to Southern California, teenage Joan threw herself into the wild Los Angeles music scene, hanging around the clubs where glam-rock kids and music-business characters mixed together. It was there she crossed paths with a record producer named Kim Fowley, and pitched him an idea that had been burning in her: a band made up entirely of girls — teenage girls — playing hard, loud rock and roll. The kind of band the world had never seen.
In 1975, that band was born. They called themselves The Runaways. Joan started it alongside a drummer named Sandy West, and soon added lead guitarist Lita Ford and bassist Jackie Fox. There was just one thing still missing.
They needed a lead singer.
They found her at a teen nightclub. Her name was Cherie Currie — fifteen years old, from the San Fernando Valley, and she strode in dripping with attitude in a David Bowie-inspired look, all lightning bolts and defiance. She had never sung with a rock band in her life. She’d come prepared to audition with the old standard “Fever” — but when she got up to sing it, nobody in the room knew how to play it.
And here is where the story becomes something special.
They didn’t send her home. Instead, Joan and Fowley ducked into the next room and did something extraordinary: they wrote her a brand-new song, on the spot, tailored to her voice, in about twenty minutes flat. Joan started hammering out a riff, the words came tumbling out — “Hello Daddy, hello Mom…” — and they walked back in and told the stunned teenager to sing it.
The song was called “Cherry Bomb.” Cherie belted it out, raw and fearless.
She had the part.
Think about the ages of these girls for a moment. Cherie was fifteen. Joan was sixteen. Every last one of them was a teenager. And together, they were about to hit the world like a fist.
In 1976, Mercury Records signed them, and the backlash was brutal. American audiences and critics did not know what to do with five teenage girls playing snarling, unapologetic rock and roll, singing openly about rebellion and freedom. At first the reaction was condescending; then, as it became clear these girls were dead serious about their music, it turned ugly. They were sneered at and insulted. Male fans hurled things at them from the crowd. Joan was struck by a beer bottle, cracked a rib, and once took a battery to the face.
They kept right on playing. Every single night.
And then, in the summer of 1977, everything flipped. The band flew to Japan — and walked straight into pandemonium.
They stepped off the plane into a wall of screaming fans, a frenzy Joan would later compare to the height of Beatlemania. In Japan, the Runaways weren’t a punchline or a novelty act. They were bona fide rock stars. They sold out huge venues. Their live album went gold. Six thousand miles from a country that had jeered at them, five teenage girls were finally treated exactly as they deserved.
But the pressures were mounting, and the cracks were beginning to show. In 1977, at just seventeen, Cherie Currie — worn down and struggling with addiction she would one day write about with unflinching honesty in her memoir, Neon Angel — walked away from the band. Her road back would be a long one. But she fought her way through it, got clean, and rebuilt her life completely — eventually working as a counselor to at-risk teenagers, and even becoming an artist who sculpts with a chainsaw. She came out the other side whole.
Joan, meanwhile, did not stop. She took over as lead singer. The Runaways made a couple more records before finally breaking up in 1979. (Sandy West, who’d started it all with Joan, remained a fierce presence in the band’s story until her death in 2006.)
And then the music industry handed Joan Jett its verdict.
Twenty-three record labels. Twenty-three rejections. Every major company passed on her. One even sent back the gutting note that maybe they’d be interested — if she’d just lose the guitar. The woman who’d co-written “Cherry Bomb” at sixteen and survived flying bottles and sold-out arenas could not get a single label to say yes.
She refused to take no for an answer.
So in 1980, together with producer Kenny Laguna, Joan Jett did something almost unheard of: she started her own label, Blackheart Records — one of the first record labels in rock history owned by a woman. They pressed the albums themselves. They sold copies out of the trunks of their cars. They built it with their own hands, from nothing, because nobody would build it for them.
And then came the vindication.
In early 1982, “I Love Rock ‘n’ Roll” roared to number one on the charts and stayed there for seven straight weeks. It became one of the defining anthems of the entire decade — a song Joan had first heard as a teenager on tour in England and instantly known, in her bones, that she would someday make her own.
In 2015, Joan Jett and the Blackhearts were inducted into the Rock and Roll Hall of Fame. She’s been named to Rolling Stone’s list of the greatest guitarists of all time — twice.
The girl an instructor once told that girls can’t play rock and roll is now, officially, recognized as one of the greatest guitarists who ever lived.
She didn’t do it alone, and she’d be the first to say so — there were trailblazing women before her, and a whole band of fearless girls beside her. But it was Joan Jett who kept swinging when the whole industry told her no. And every woman who has picked up an electric guitar since has walked through a door that she, and the girls beside her, kicked wide open.

Their internal numbers reveal catastrophic spikes in serious conditions:
• 487% spike in Breast Cancer
• 369% spike in Testicular Cancer
• 2181% spike in Hypertension
• 680% spike in Multiple Sclerosis
• 551% spike in Guillain-Barré Syndrome
And many more.
This is not speculation — it’s straight from their own reported data.
Independent studies have also raised serious concerns:
– Fatal Myocarditis: A 2024 systematic review of autopsies found a causal link between COVID-19 vaccines and fatal myocarditis in multiple cases (Hulscher et al., ESC Heart Failure).
– Cancer: A large 2025 South Korean population study (Kim et al.) found significantly increased 1-year risks of several cancers post-vaccination.
– Excess Deaths: A major Japanese analysis showed excess deaths occurred ONLY in the COVID-vaccinated group, with no excess deaths observed in the unvaccinated.
The buried TRUTH is coming out…

You may have missed this when it was published a few years ago. I think it is worth listening to in the current peaceful break between storms.
Click to view the video: https://www.facebook.com/reel/205101768124720
You might not be aware that you are in a daily battle to retain your health, but you are.
“Fat is bad, eat more grains.”
Except fats are vital to transport fat
soluble vitamins in the body and obesity
rates have since exploded.
No conflict here, move along please.
Remove the toxic conflicts from your life.
Stabilize the front line and reclaim lost territory.
Aim for food peace and bodily health.
Eat real ingredients.
www.fulvicminerals.com.au
www.healthelicious.com.au
www.howtolivethehealthiestlife.com.au
www.yourgreens.com.au
You might not be aware that you are in a daily battle to retain your health, but you are.
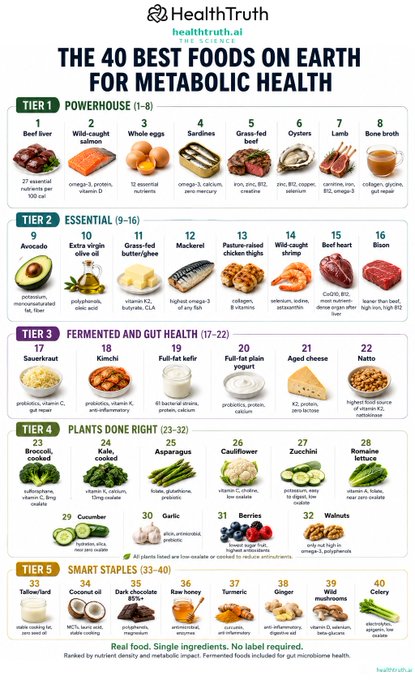
I posted the 20 best foods on earth. Many people saw it. The reply section exploded.
The carnivores said I included too many vegetables. The plant-based crowd said I included too much meat. Someone told me spinach was poisoning people. Someone else told me I should be in jail for recommending beef liver.
I listened to all of it. Went back to the data. This is Version 2. 40 foods. Updated.
Spinach is gone. Fermented foods are in. Organ meats expanded. Every plant on this list is low-oxalate or cooked to reduce antinutrients.
No tribe won. The science won.
Finish reading: https://x.com/markkaplan20/status/2079906122451018090?s=20
Some reports estimate that moms are interrupted every three minutes—hundreds of times each day. Whether the exact number is 200 or 400, every parent knows the feeling.
Each interruption forces your brain to pause, switch gears, and start over. Research shows that frequent interruptions increase cognitive load, reduce working memory, and raise stress levels. So if you’ve ever walked into a room and forgotten why, lost your train of thought mid-sentence, or felt mentally drained before lunch, you’re not imagining it.
Motherhood isn’t just physically demanding. It’s one of the most cognitively demanding jobs there is. So if you’re raising little humans while juggling a hundred invisible tasks, give yourself some grace. Your brain isn’t broken—it’s been asked to do the impossible all day long.